Helleberg Marie, May Margaret T, Ingle Suzanne M, Dabis Francois, Reiss Peter, Fätkenheuer Gerd, Costagliola Dominique, d'Arminio Antonella, Cavassini Matthias, Smith Colette, Justice Amy C, Gill John, Sterne Jonathan A C, Obel Niels
aDepartment of Infectious Diseases, Copenhagen University Hospital, Rigshospitalet bFaculty of Health Sciences, University of Copenhagen, Copenhagen, Denmark cSchool of Social and Community Medicine, University of Bristol, Bristol, UK dUniversité Bordeaux, ISPED, Centre INSERM U897-Epidémiologie-Biostatistique, Bordeaux, France eDepartment of Global Health, Academisch Medisch Centrum bij de Universiteit van Amsterdam, and Stichting HIV Monitoring, Amsterdam, The Netherlands fDepartment of Internal Medicine, University of Cologne and German Centre for Infection Research (DZIF), Cologne, Germany gSorbonne Universités, UPMC Univ Paris 06 hINSERM, UMR_S 1136, Institut Pierre Louis d'Epidémiologie et de Santé Publique, Paris, France iClinic of Infectious Diseases & Tropical Medicine, San Paolo Hospital, University of Milan, Milan, Italy jService des maladies infectieuses, CHUV, Lausanne, Switzerland kResearch Department of Infection and Population Health, University College London, London, UK lYale University, New Haven mVA Connecticut Healthcare System, West Haven, Connecticut, USA nDivision of Infectious Diseases, University of Calgary, Calgary, Alberta, Canada.
AIDS. 2015 Jan 14;29(2):221-9. doi: 10.1097/QAD.0000000000000540.
Cardiovascular disease and non-AIDS malignancies have become major causes of death among HIV-infected individuals. The relative impact of lifestyle and HIV-related factors are debated.
We estimated associations of smoking with mortality more than 1 year after antiretroviral therapy (ART) initiation among HIV-infected individuals enrolled in European and North American cohorts. IDUs were excluded. Causes of death were assigned using standardized procedures. We used abridged life tables to estimate life expectancies. Life-years lost to HIV were estimated by comparison with the French background population.
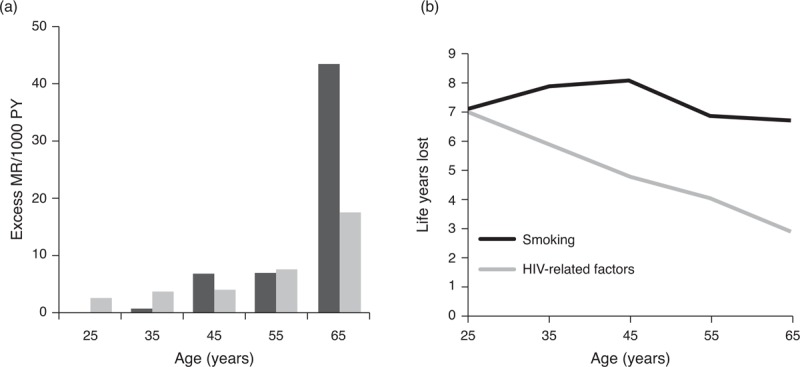
Among 17,995 HIV-infected individuals followed for 79,760 person-years, the proportion of smokers was 60%. The mortality rate ratio (MRR) comparing smokers with nonsmokers was 1.94 [95% confidence interval (95% CI) 1.56-2.41]. The MRRs comparing current and previous smokers with never smokers were 1.70 (95% CI 1.23-2.34) and 0.92 (95% CI 0.64-1.34), respectively. Smokers had substantially higher mortality from cardiovascular disease, non-AIDS malignancies than nonsmokers [MRR 6.28 (95% CI 2.19-18.0) and 3.31 (95% CI 1.80-5.45), respectively]. [corrected]. Among 35-year-old HIV-infected men, the loss of life-years associated with smoking and HIV was 7.9 (95% CI 7.1-8.7) and 5.9 (95% CI 4.9-6.9), respectively. The life expectancy of virally suppressed, never-smokers was 43.5 years (95% CI 41.7-45.3), compared with 44.4 years among 35-year-old men in the background population. Excess MRRs/1000 person-years associated with smoking increased from 0.6 (95% CI -1.3 to 2.6) at age 35 to 43.6 (95% CI 37.9-49.3) at age at least 65 years.
Well treated HIV-infected individuals may lose more life years through smoking than through HIV. Excess mortality associated with smoking increases markedly with age. Therefore, increases in smoking-related mortality can be expected as the treated HIV-infected population ages. Interventions for smoking cessation should be prioritized.
心血管疾病和非艾滋病相关恶性肿瘤已成为HIV感染者的主要死因。生活方式和HIV相关因素的相对影响存在争议。
我们评估了在欧洲和北美队列中登记的HIV感染者开始抗逆转录病毒治疗(ART)1年多后吸烟与死亡率之间的关联。排除注射吸毒者。使用标准化程序确定死因。我们使用简略生命表来估计预期寿命。通过与法国背景人群比较来估计因HIV导致的生命年损失。
在17995名接受随访79760人年的HIV感染者中,吸烟者比例为60%。吸烟者与非吸烟者的死亡率比(MRR)为1.94[95%置信区间(95%CI)1.56 - 2.41]。当前吸烟者和既往吸烟者与从不吸烟者相比的MRR分别为1.70(95%CI 1.23 - 2.34)和0.92(95%CI 0.64 - 1.34)。吸烟者死于心血管疾病、非艾滋病相关恶性肿瘤的死亡率显著高于非吸烟者[MRR分别为6.28(95%CI 2.19 - 18.0)和3.31(95%CI 1.80 - 5.45)]。[已校正]。在35岁的HIV感染男性中,与吸烟和HIV相关的生命年损失分别为7.9(95%CI 7.1 - 8.7)和5.9(95%CI 4.9 - 6.9)。病毒得到抑制的从不吸烟者的预期寿命为43.5岁(95%CI 41.7 - 45.3),而背景人群中35岁男性的预期寿命为44.4岁。与吸烟相关的每1000人年额外MRR从35岁时的0.6(95%CI -1.3至2.6)增加到至少65岁时的43.6(95%CI 37.9 - 49.3)。
接受良好治疗的HIV感染者因吸烟可能比因HIV失去更多生命年。与吸烟相关的额外死亡率随年龄显著增加。因此,随着接受治疗的HIV感染人群老龄化,与吸烟相关的死亡率预计会上升。应优先考虑戒烟干预措施。