Bock Dirk E, Robinson Tracy, Seabrook Jamie A, Rombeek Meghan, Norozi Kambiz, Filler Guido, Rauch Ralf, Clarson Cheril L
Department of Pediatrics, Children's Hospital, London Health Sciences Centre, Western University, 800 Commissioners Road East, London, ON, N6A 5W9, Canada.
Lawson Health Research Institute, 750 Base Line Road, Suite 300, London, ON, N6C 2R5, Canada.
BMC Pediatr. 2014 Dec 5;14:296. doi: 10.1186/s12887-014-0296-1.
Though recent data suggest that multidisciplinary outpatient interventions can have a positive effect on childhood obesity, it is still unclear which program components are most beneficial and how they affect quality of life (QoL). The aim of this study was to determine if a 1-year multidisciplinary, family-centered outpatient intervention based on social cognitive theory would be effective in (i) preventing further increases in BMI and BMI z-score, and (ii) improving QoL in obese children and adolescents.
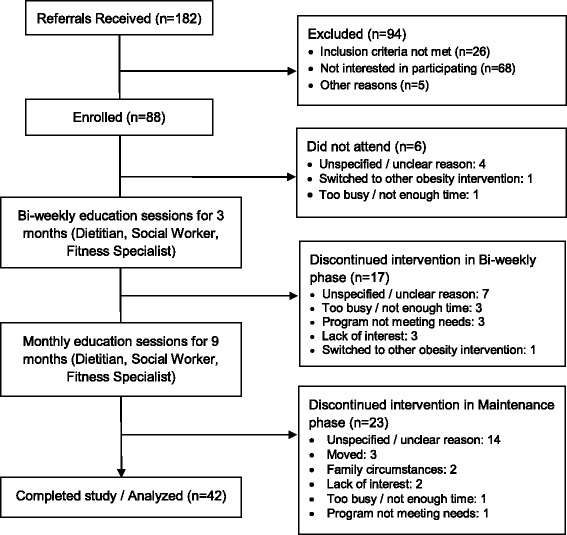
Obese children and adolescents 8-17 years of age and their families participated in this 1-year longitudinal pilot intervention study. The intervention consisted of fifteen 90-minute educational sessions led by a dietitian, exercise specialist, and social worker. Anthropometric measures, body composition, and QoL (Pediatric Quality of Life Inventory 4.0), were assessed at baseline, 3 months, and 12 months. Laboratory values were measured at baseline and 12 months. The primary outcome measures were change in BMI and BMI z-score, secondary outcome measures included change in QoL and body composition. A paired sample t-test was used to assess within-group differences and 95% confidence intervals were reported for the mean differences.
42 obese children and adolescents (21 girls) completed the 1-year intervention (mean age 12.8 ± 3.14 years). Mean baseline BMI was 31.96 ± 5.94 kg/m(2) and BMI z-score was +2.19 ± 0.34. Baseline QoL (self-assessments and parental assessments) was impaired: mean baseline scores were 74.5 ± 16.5 and 63.7 ± 19.4 for physical functioning and 69.0 ± 14.9 and 64.0 ± 18.3 for emotional functioning, respectively. At 12 months, BMI z-score had decreased (-0.07 ± 0.11, 95% CI: -0.11 to -0.04). BMI (0.80 ± 1.57 kg/m(2), 95% CI 0.31 to 1.29) and fat-free mass (4.02 ± 6.27 kg, 95% CI 1.90 to 6.14) increased, but % body fat and waist circumference did not. Both the parent-reported physical (11.3 ± 19.2, 95% CI 4.7 to 17.9) and emotional (7.7 ± 15.7, 95% CI 2.3 to 13.0) functioning QoL scores and the children's self-reported physical (5.3 ± 17.1, 95% CI 0.5 to 11.1) and emotional (7.9 ± 14.3, 95% CI 3.2 to 12.7) functioning scores significantly improved.
Following a 1-year intervention, the participants' BMI z-scores and QoL improved, while other adiposity-related measures of body composition remained unchanged.
UMIN Clinical Trials Registry UMIN000015622 .
尽管近期数据表明多学科门诊干预对儿童肥胖症可能产生积极影响,但仍不清楚哪些项目组成部分最有益以及它们如何影响生活质量(QoL)。本研究的目的是确定基于社会认知理论的为期1年的多学科、以家庭为中心的门诊干预是否能有效(i)防止体重指数(BMI)和BMI z评分进一步升高,以及(ii)改善肥胖儿童和青少年的生活质量。
8至17岁的肥胖儿童和青少年及其家庭参与了这项为期1年的纵向试点干预研究。干预包括由营养师、运动专家和社会工作者主持的15次90分钟的教育课程。在基线、3个月和12个月时评估人体测量指标、身体成分和生活质量(儿童生活质量量表4.0)。在基线和12个月时测量实验室值。主要结局指标是BMI和BMI z评分的变化,次要结局指标包括生活质量和身体成分的变化。采用配对样本t检验评估组内差异,并报告平均差异的95%置信区间。
42名肥胖儿童和青少年(21名女孩)完成了为期1年的干预(平均年龄12.8±3.14岁)。平均基线BMI为31.96±5.94kg/m²,BMI z评分为+2.19±0.34。基线生活质量(自我评估和家长评估)受损:身体功能的平均基线评分分别为74.5±16.5和63.7±19.4,情感功能的平均基线评分分别为69.0±14.9和64.0±18.3。在12个月时,BMI z评分下降(-0.07±0.11,95%置信区间:-0.11至-0.04)。BMI(0.80±1.57kg/m²,95%置信区间0.31至1.29)和去脂体重(4.02±6.27kg,95%置信区间1.90至6.14)增加,但体脂百分比和腰围没有变化。家长报告的身体(11.3±19.2,95%置信区间4.7至17.9)和情感(7.7±15.7,95%置信区间2.3至13.0)功能生活质量评分以及儿童自我报告的身体(5.3±17.1,95%置信区间0.5至11.1)和情感(7.9±14.3,95%置信区间3.2至12.7)功能评分均显著改善。
经过1年的干预,参与者的BMI z评分和生活质量得到改善,而其他与肥胖相关的身体成分指标保持不变。
UMIN临床试验注册中心UMIN000015622 。