Kirkpatrick Andrew W, Roberts Derek J, Faris Peter D, Ball Chad G, Kubes Paul, Tiruta Corina, Xiao Zhengwen, Holodinsky Jessalyn K, McBeth Paul B, Doig Christopher J, Jenne Craig N
*Department of Surgery, University of Calgary and the Foothills Medical Centre, Calgary, Alberta, Canada †Regional Trauma Program, University of Calgary and the Foothills Medical Centre, Calgary, Alberta, Canada ‡Department of Community Health Sciences, University of Calgary, TRW (Teaching, Research, and Wellness), Calgary, Alberta, Canada §Department of Critical Care Medicine, University of Calgary, Calgary, Alberta, Canada ¶Alberta Health Services-Research Excellence Support Team, University of Calgary and the Foothills Medical Centre, Calgary, Alberta, Canada ‖Department of Oncology, University of Calgary and the Foothills Medical Centre, Calgary, Alberta, Canada **Department of Microbiology, Immunology, and Infectious Diseases, University of Calgary, Calgary, Alberta, Canada ††Calvin, Phoebe, and Joan Snyder Institute for Chronic Diseases, University of Calgary, Health Research Innovation Centre, Calgary, Alberta, Canada; and ‡‡Hotchkiss Brain Institute, University of Calgary and the Foothills Medical Centre, Health Research Innovation Centre, Calgary, Alberta, Canada.
Ann Surg. 2015 Jul;262(1):38-46. doi: 10.1097/SLA.0000000000001095.
To determine whether active negative pressure peritoneal therapy with the ABThera temporary abdominal closure device reduces systemic inflammation after abbreviated laparotomy.
Excessive systemic inflammation after abdominal injury or intra-abdominal sepsis is associated with poor outcomes.
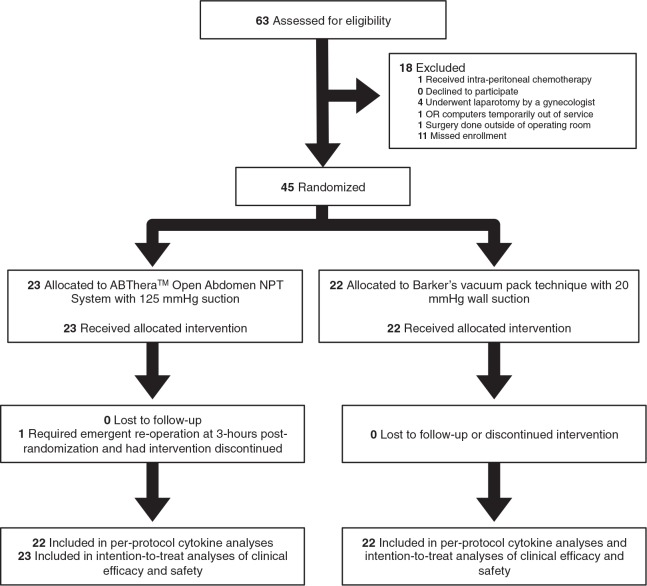
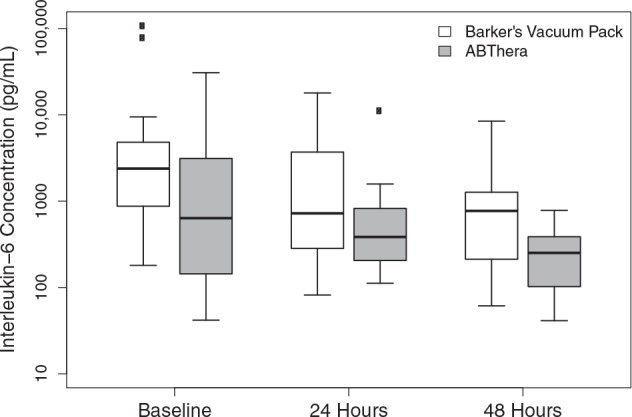
We conducted a single-center, randomized controlled trial. Forty-five adults with abdominal injury (46.7%) or intra-abdominal sepsis (52.3%) were randomly allocated to the ABThera (n = 23) or Barker's vacuum pack (n = 22). On study days 1, 2, 3, 7, and 28, blood and peritoneal fluid were collected. The primary endpoint was the difference in the plasma concentration of interleukin-6 (IL-6) 24 and 48 hours after temporary abdominal closure application.
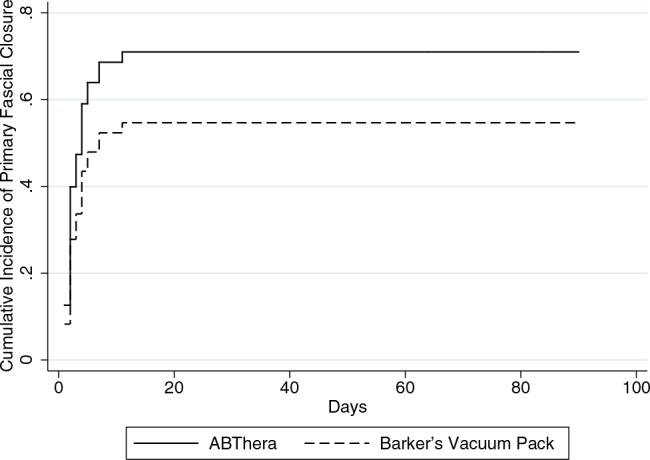
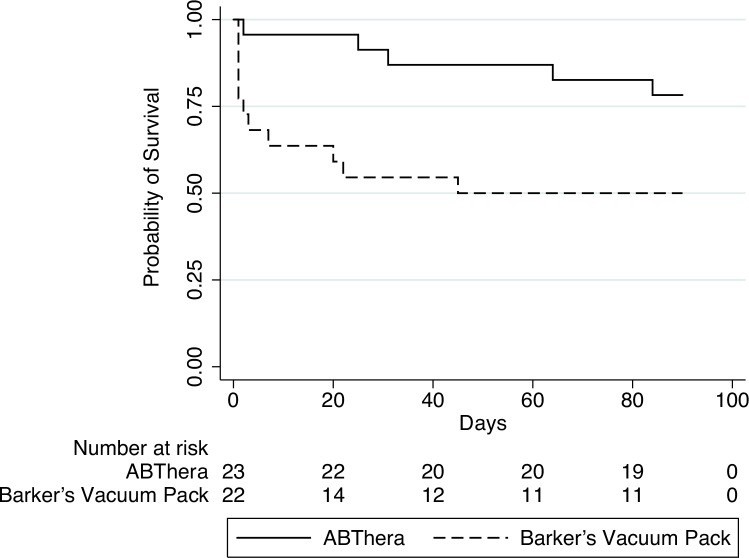
There was a significantly lower peritoneal fluid drainage from the ABThera at 48 hours after randomization. Despite this, there was no difference in plasma concentration of IL-6 at baseline versus 24 (P = 0.52) or 48 hours (P = 0.82) between the groups. There was also no significant intergroup difference in the plasma concentrations of IL-1β, -8, -10, or -12 p70 or tumor necrosis factor α between these time points. The cumulative incidence of primary fascial closure at 90 days was similar between groups (hazard ratio, 1.6; 95% confidence interval, 0.82-3.0; P = 0.17). However, 90-day mortality was improved in the ABThera group (hazard ratio, 0.32; 95% confidence interval, 0.11-0.93; P = 0.04).
This trial observed a survival difference between patients randomized to the ABThera versus Barker's vacuum pack that did not seem to be mediated by an improvement in peritoneal fluid drainage, fascial closure rates, or markers of systemic inflammation.
ClinicalTrials.gov identifier NCT01355094.
确定使用ABThera临时腹部闭合装置进行主动负压腹膜治疗是否能减轻简化剖腹术后的全身炎症反应。
腹部损伤或腹腔内脓毒症后过度的全身炎症反应与不良预后相关。
我们进行了一项单中心随机对照试验。45例腹部损伤患者(46.7%)或腹腔内脓毒症患者(52.3%)被随机分配至ABThera组(n = 23)或Barker真空包装组(n = 22)。在研究的第1、2、3、7和28天,采集血液和腹腔液。主要终点是临时腹部闭合应用后24小时和48小时白细胞介素-6(IL-6)血浆浓度的差异。
随机分组后48小时,ABThera组的腹腔液引流量显著更低。尽管如此,两组间基线时与24小时(P = 0.52)或48小时(P = 0.82)的IL-6血浆浓度并无差异。在这些时间点之间,两组间IL-1β、-8、-10或-12 p70的血浆浓度以及肿瘤坏死因子α也无显著组间差异。90天时一期筋膜闭合的累积发生率在两组间相似(风险比,1.6;95%置信区间,0.82 - 3.0;P = 0.17)。然而,ABThera组的90天死亡率有所改善(风险比,0.32;95%置信区间,0.11 - 0.93;P = 0.04)。
本试验观察到,随机分配至ABThera组与Barker真空包装组的患者之间存在生存差异,这似乎并非由腹腔液引流量的改善、筋膜闭合率或全身炎症标志物的改善所介导。
ClinicalTrials.gov标识符NCT01355094。