Ruan Yue, Elleri Daniela, Allen Janet M, Tauschmann Martin, Wilinska Malgorzata E, Dunger David B, Hovorka Roman
Department of Paediatrics, University of Cambridge, Cambridge, UK.
Diabetologia. 2015 Apr;58(4):687-90. doi: 10.1007/s00125-014-3483-6. Epub 2014 Dec 24.
AIMS/HYPOTHESIS: The aim of this study was to compare the pharmacokinetics of two different concentrations of insulin aspart (B28Asp human insulin) in children aged 3-6 years with type 1 diabetes.
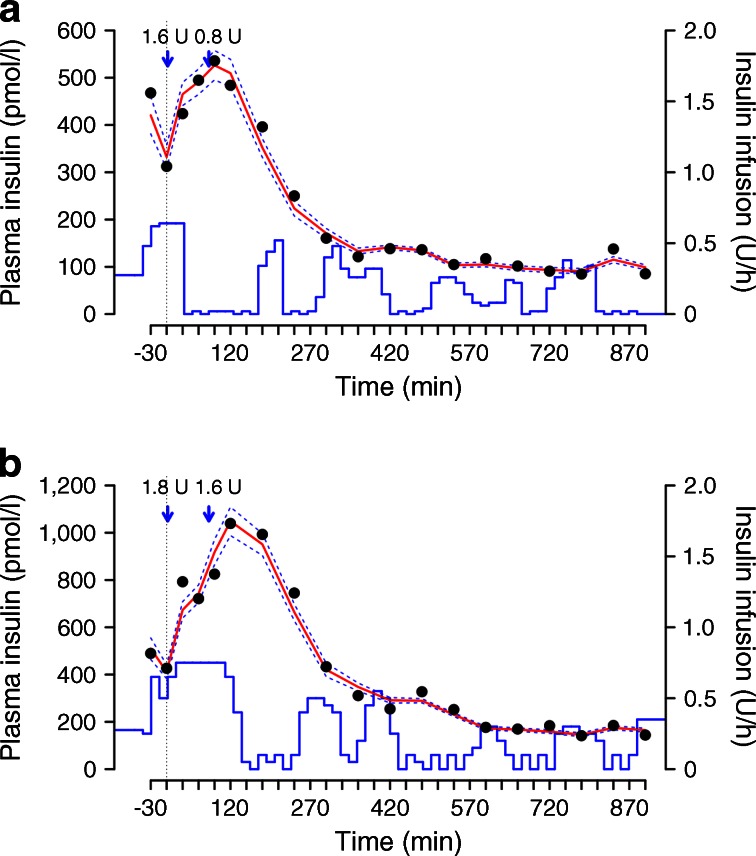
Young children with type 1 diabetes underwent an open-label, randomised, two-period crossover study in a clinical research facility, 2-6 weeks apart. In random order, diluted (1:5 dilution with saline [154 mmol/l NaCl]; 20 U/ml) or standard strength (100 U/ml) insulin aspart was administered via an insulin pump as a meal bolus and then overnight by closed-loop insulin delivery as determined by a model predictive algorithm. Plasma insulin was measured every 30-60 min from 17:00 hours on day 1 to 8:00 hours on day 2. We measured the time-to-peak insulin concentration (tmax), insulin metabolic clearance rate (MCR(I)) and background insulin concentration (ins(c)) using compartmental modelling.
Eleven children (six male; age range 3.75-6.96 years, HbA1c 7.6% ± 1.3% [60 ± 14 mmol/mol], BMI standard deviation score 1.0 ± 0.8, duration of diabetes 2.2 ± 1.0 years, total daily dose 12.9 [10.6-16.5] U, fasting C-peptide concentration 5 [5-17.1] pmol/l; mean ± SD or median [interquartile range]) participated in the study. No differences between standard and diluted insulin were observed in terms of t max (59.2 ± 14.4 vs 61.6 ± 8.7) min for standard vs diluted, p = 0.59; MCR I (1.98 × 10(-2) ± 0.99 × 10(-2) vs 1.89 × 10(-2) ± 0.82 × 10(-2) 1/kg/min, p = 0.47), and ins c (34 [1-72] vs 23 [3-65] pmol/l, p = 0.66). However, t max showed less intersubject variability following administration of diluted aspart (SD 14.4 vs 8.7 min, p = 0.047).
CONCLUSIONS/INTERPRETATION: Diluting insulin aspart does not change its pharmacokinetics. However, it may result in less variable absorption and could be used in young children with type 1 diabetes undergoing closed-loop insulin delivery.
Clinicaltrials.gov NCT01557634.
FUNDING was provided by the JDRF, 7th Framework Programme of the European Union, Wellcome Trust Strategic Award and the National Institute for Health Research Cambridge Biomedical Research Centre.
目的/假设:本研究旨在比较两种不同浓度的门冬胰岛素(B28Asp人胰岛素)在3至6岁1型糖尿病儿童中的药代动力学。
1型糖尿病幼儿在临床研究机构进行了一项开放标签、随机、两期交叉研究,两期间隔2至6周。按照随机顺序,通过胰岛素泵给予稀释(用生理盐水[154 mmol/l NaCl] 1:5稀释;20 U/ml)或标准浓度(100 U/ml)的门冬胰岛素作为餐时大剂量注射,然后根据模型预测算法通过闭环胰岛素输注进行夜间给药。从第1天17:00至第2天8:00每30 - 60分钟测量一次血浆胰岛素。我们使用房室模型测量胰岛素峰值浓度时间(tmax)、胰岛素代谢清除率(MCR(I))和基础胰岛素浓度(ins(c))。
11名儿童(6名男性;年龄范围3.75 - 6.96岁,糖化血红蛋白7.6% ± 1.3% [60 ± 14 mmol/mol],BMI标准差评分1.0 ± 0.8,糖尿病病程2.2 ± 1.0年,每日总剂量12.9 [10.6 - 16.5] U,空腹C肽浓度5 [5 - 17.1] pmol/l;均值 ± 标准差或中位数[四分位间距])参与了研究。标准与稀释胰岛素在tmax方面未观察到差异(标准组为59.2 ± 14.4分钟,稀释组为61.6 ± 8.7分钟,p = 0.59);MCR I(1.98×10(-2) ± 0.99×10(-2) 与1.89×10(-2) ± 0.82×10(-2) 1/kg/min,p = 0.47),以及ins c(34 [1 - 72] 与23 [3 - 65] pmol/l,p = 0.66)。然而,给予稀释门冬胰岛素后tmax的个体间变异性较小(标准差14.4与8.7分钟,p = 0.047)。
结论/解读:稀释门冬胰岛素不会改变其药代动力学。然而,它可能导致吸收变异性较小,可用于接受闭环胰岛素输注的1型糖尿病幼儿。
Clinicaltrials.gov NCT01557634。
由青少年糖尿病研究基金会、欧盟第七框架计划、惠康信托战略奖以及国家卫生研究院剑桥生物医学研究中心提供资助。