Calder Lisa, Pozgay Anita, Riff Shena, Rothwell David, Youngson Erik, Mojaverian Naghmeh, Cwinn Adam, Forster Alan
Department of Emergency Medicine, University of Ottawa, Ottawa, Ontario, Canada Clinical Epidemiology Program, Ottawa Hospital Research Institute, Ottawa, Ontario, Canada.
Department of Emergency Medicine, University of Ottawa, Ottawa, Ontario, Canada.
BMJ Qual Saf. 2015 Feb;24(2):142-8. doi: 10.1136/bmjqs-2014-003194. Epub 2014 Dec 24.
This study describes the proportion of emergency department (ED) returns within 7 days due to adverse events, defined as adverse outcomes related to healthcare received.
Prospective cohort study.
We used an electronically triggered adverse event surveillance system at a tertiary care ED from May to June 2010 to examine ED returns within 7 days of index visit.
One of three trained nurses determined whether the visit was related to index emergency care. For such records, one of three trained emergency physicians conducted adverse event determinations.
We determined adverse event type and severity and analysed the data with descriptive statistics, χ(2) tests and logistic regression.
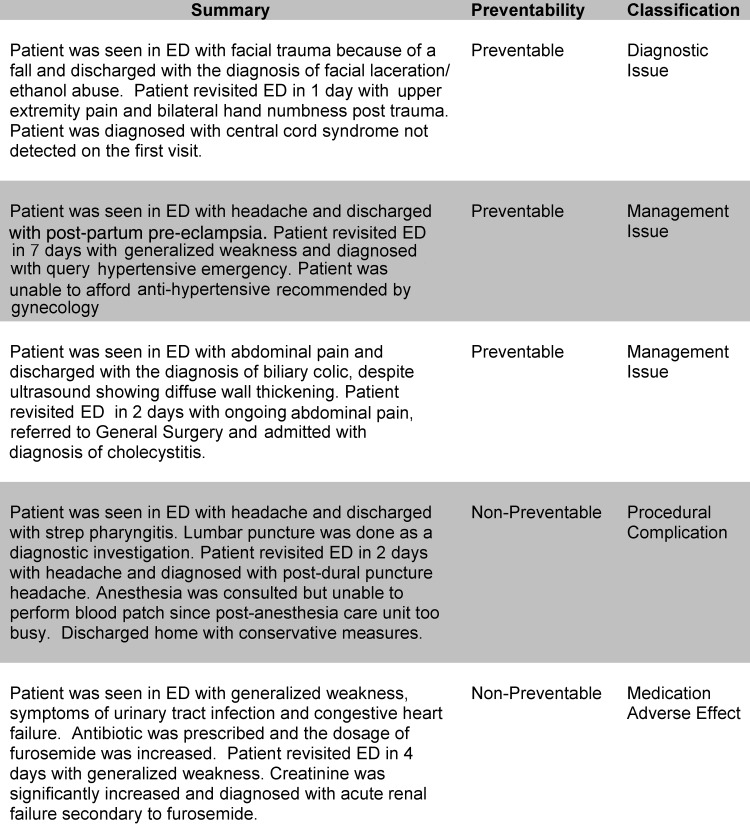
Of 13,495 index ED visits, 923 (6.8%) were followed by ED returns within 7 days. The median age of all patients was 47 years and 52.8% were women. After nursing review, 211 cases required physician review. Of these, 53 visits were adverse events (positive predictive value (PPV)=5.7%, 95% CI 4.4% to 7.4%) and 30 (56.6%) were preventable. Common adverse event types involved management, diagnostic or medication issues. We observed one potentially preventable death and 58.5% of adverse events resulting in transient disability. The PPV of a modified trigger with a cut-off of return within 72 h, resulting in admission was 11.9% (95% CI 6.8% to 18.9%).
Our electronic trigger efficiently identified adverse events among 12% of patients with ED returns within 72 h, requiring hospital admission. Given the high degree of preventability of the identified adverse events, this trigger also holds promise as a performance measurement tool.
本研究描述了因不良事件导致的7天内急诊科(ED)复诊比例,不良事件定义为与所接受医疗保健相关的不良后果。
前瞻性队列研究。
我们于2010年5月至6月在一家三级护理急诊科使用电子触发的不良事件监测系统,以检查首次就诊后7天内的急诊科复诊情况。
三名经过培训的护士之一确定此次就诊是否与首次急诊护理相关。对于此类记录,三名经过培训的急诊医生之一进行不良事件判定。
我们确定了不良事件的类型和严重程度,并使用描述性统计、χ²检验和逻辑回归分析数据。
在13495例首次急诊科就诊患者中,923例(6.8%)在7天内进行了急诊科复诊。所有患者的中位年龄为47岁,52.8%为女性。经过护理评估后,211例病例需要医生评估。其中有53次就诊为不良事件(阳性预测值(PPV)=5.7%,95%可信区间4.4%至7.4%),30例(56.6%)是可预防的。常见的不良事件类型涉及管理、诊断或用药问题。我们观察到1例潜在可预防的死亡,58.5%的不良事件导致短暂残疾。72小时内复诊并导致入院的改良触发指标的PPV为11.9%(95%可信区间6.8%至18.9%)。
我们的电子触发指标有效地在需住院治疗的72小时内急诊科复诊患者中的12%中识别出不良事件。鉴于所识别不良事件的高度可预防性,该触发指标也有望成为一种绩效衡量工具。