Best Kaitlin M, Boullata Joseph I, Curley Martha A Q
1School of Nursing, University of Pennsylvania, Philadelphia, PA. 2Department of Biobehavioral Health Sciences, School of Nursing, University of Pennsylvania, Philadelphia, PA. 3Department of Family & Community Heath, School of Nursing, Philadelphia, PA.
Pediatr Crit Care Med. 2015 Feb;16(2):175-83. doi: 10.1097/PCC.0000000000000306.
Analgesia and sedation are common therapies in pediatric critical care, and rapid titration of these medications is associated with iatrogenic withdrawal syndrome. We performed a systematic review of the literature to identify all common and salient risk factors associated with iatrogenic withdrawal syndrome and build a conceptual model of iatrogenic withdrawal syndrome risk in critically ill pediatric patients.
Multiple databases, including PubMed/Medline, EMBASE, CINAHL, and the Cochrane Central Registry of Clinical Trials, were searched using relevant terms from January 1, 1980, to August 1, 2014.
Articles were included if they were published in English and discussed iatrogenic withdrawal syndrome following either opioid or benzodiazepine therapy in children in acute or intensive care settings. Articles were excluded if subjects were neonates born to opioid- or benzodiazepine-dependent mothers, children diagnosed as substance abusers, or subjects with cancer-related pain; if data about opioid or benzodiazepine treatment were not specified; or if primary data were not reported.
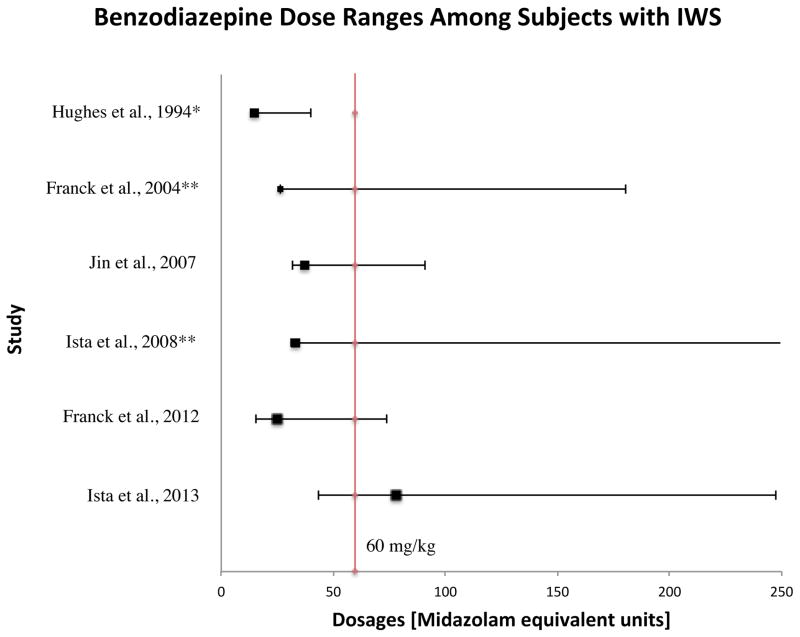
In total, 1,395 articles were evaluated, 33 of which met the inclusion criteria. To facilitate analysis, all opioid and/or benzodiazepine doses were converted to morphine or midazolam equivalents, respectively. A table of evidence was developed for qualitative analysis of common themes, providing a framework for the construction of a conceptual model. The strongest risk factors associated with iatrogenic withdrawal syndrome include duration of therapy and cumulative dose. Additionally, evidence exists linking patient, process, and system factors in the development of iatrogenic withdrawal syndrome.
Most articles were prospective observational or interventional studies.
Given the state of existing evidence, well-designed prospective studies are required to better characterize iatrogenic withdrawal syndrome in critically ill pediatric patients. This review provides data to support the construction of a conceptual model of iatrogenic withdrawal syndrome risk that, if supported, could be useful in guiding future research.
镇痛和镇静是儿科重症监护中的常见治疗方法,而这些药物的快速滴定与医源性戒断综合征相关。我们对文献进行了系统综述,以确定与医源性戒断综合征相关的所有常见且显著的风险因素,并构建危重症儿科患者医源性戒断综合征风险的概念模型。
使用相关术语检索了多个数据库,包括PubMed/Medline、EMBASE、CINAHL以及Cochrane临床试验中央注册库,检索时间范围为1980年1月1日至2014年8月1日。
纳入以英文发表且讨论急性或重症监护环境下儿童使用阿片类药物或苯二氮䓬类药物治疗后医源性戒断综合征的文章。如果研究对象是阿片类药物或苯二氮䓬类药物依赖母亲所生的新生儿、被诊断为药物滥用者的儿童或患有癌症相关疼痛的患者;如果未明确阿片类药物或苯二氮䓬类药物治疗的数据;或者未报告原始数据,则排除这些文章。
总共评估了1395篇文章,其中33篇符合纳入标准。为便于分析,所有阿片类药物和/或苯二氮䓬类药物剂量分别转换为吗啡或咪达唑仑等效剂量。编制了证据表以对常见主题进行定性分析,为构建概念模型提供框架。与医源性戒断综合征相关的最强风险因素包括治疗持续时间和累积剂量。此外,有证据表明患者、过程和系统因素与医源性戒断综合征的发生有关。
大多数文章是前瞻性观察性或干预性研究。
鉴于现有证据的情况,需要设计良好的前瞻性研究来更好地描述危重症儿科患者的医源性戒断综合征。本综述提供的数据支持构建医源性戒断综合征风险的概念模型,如果得到证实,该模型可能有助于指导未来的研究。