George Institute for Global Health, University of Oxford, Oxford OX1 3DB, UK
Centre for Statistics in Medicine, Nuffield Department of Orthopaedics, Rheumatology and Musculoskeletal Sciences, University of Oxford, Oxford, UKJ Faculty of Medicine, University of Toronto, Toronto, ON, Canada.
BMJ. 2015 Jan 28;350:h117. doi: 10.1136/bmj.h117.
To determine whether an association exists between the number of published randomised controlled trials and the global burden of disease, whether certain diseases are under-investigated relative to their burden, and whether the relation between the output of randomised trials and global burden of disease can be explained by the relative disease burden in high and low income regions.
Cross sectional investigation.
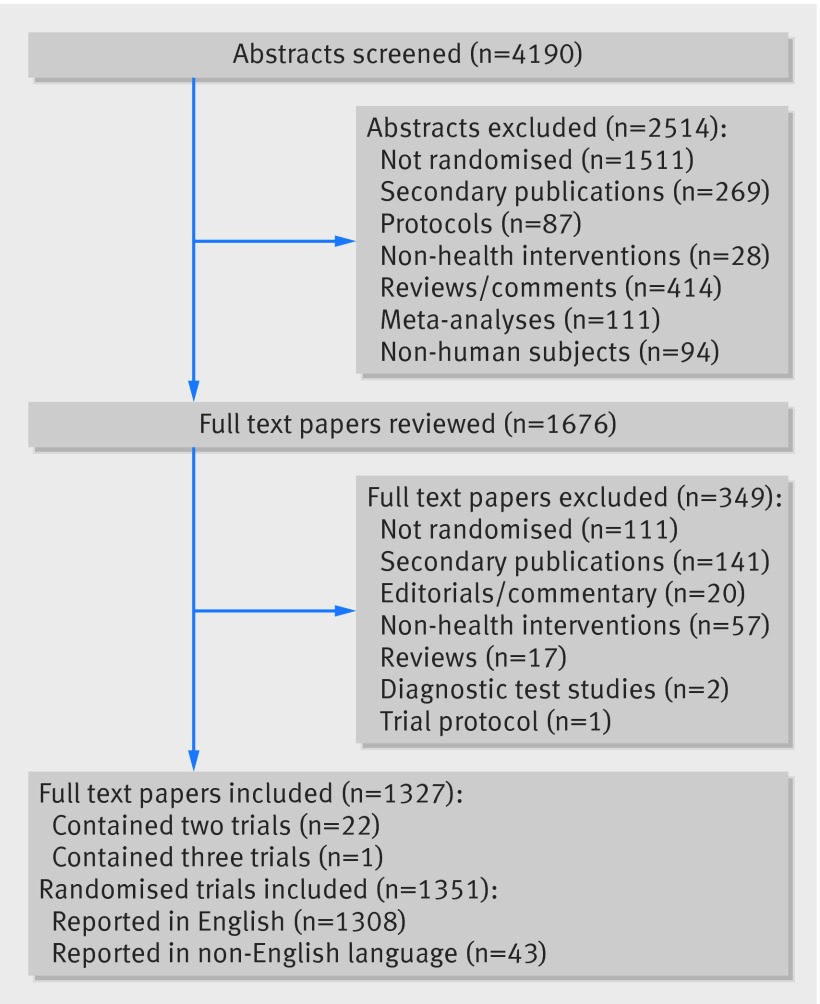
All primary reports of randomised trials published in December 2012 and indexed in PubMed by 17 November 2013.
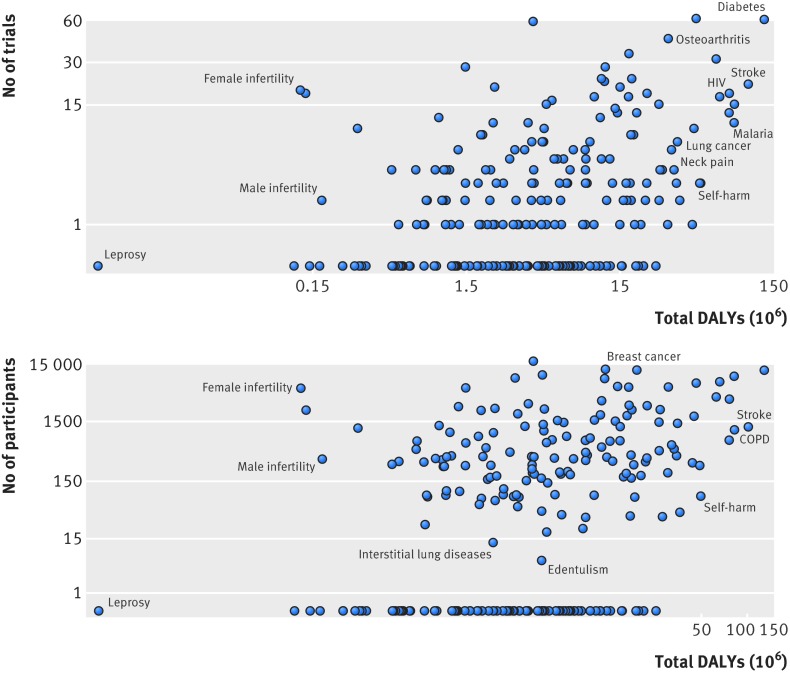
Number of trials conducted and number of participants randomised for each of 239 different diseases or injuries; variation in each outcome explainable by total disability adjusted life years (a measure of the overall burden of each disease) and the ratio of disability adjusted life years in low income to high income regions (a measure of whether a disease is more likely to affect people living in high income regions) quantified using multivariable regression.
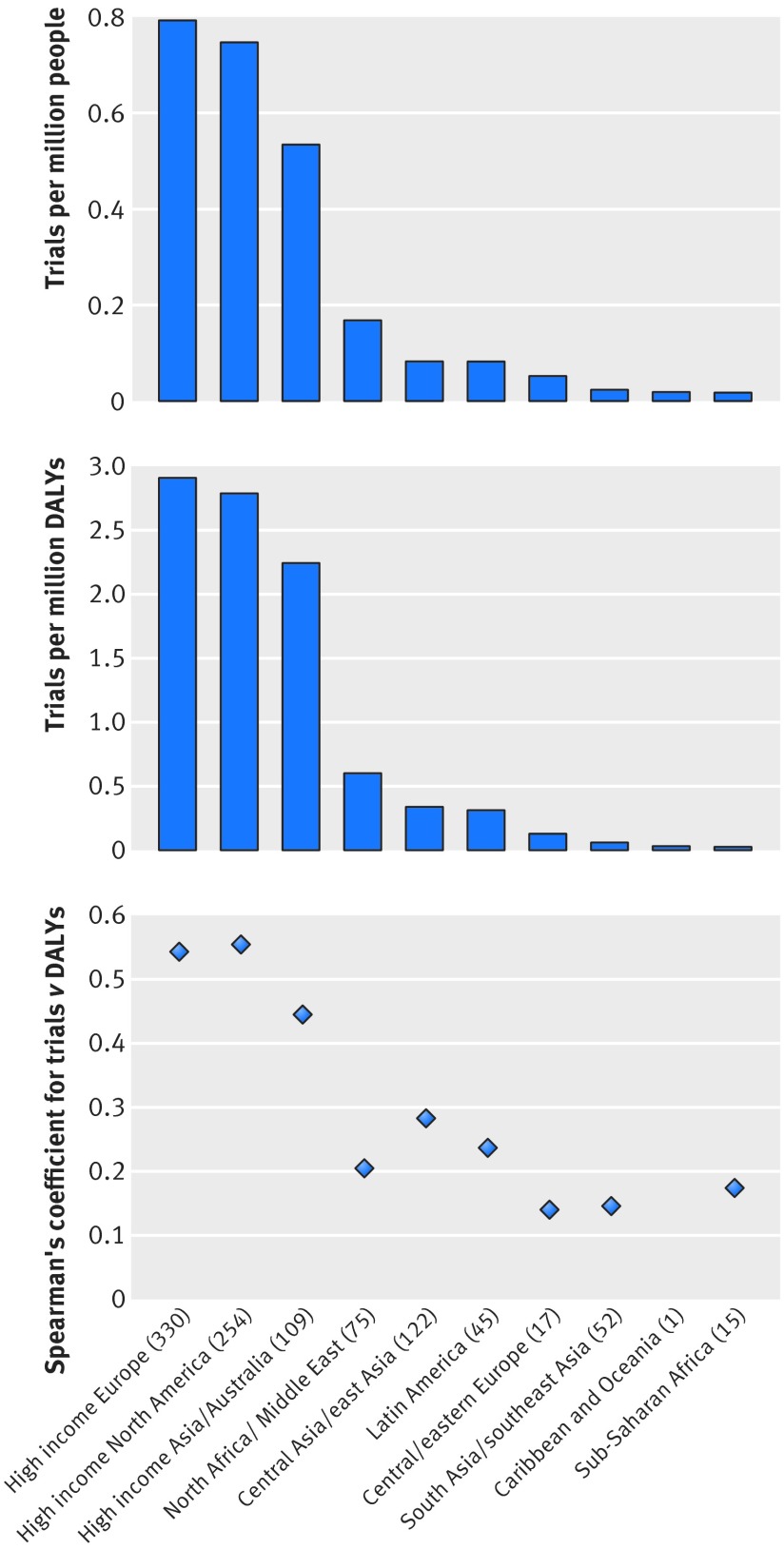
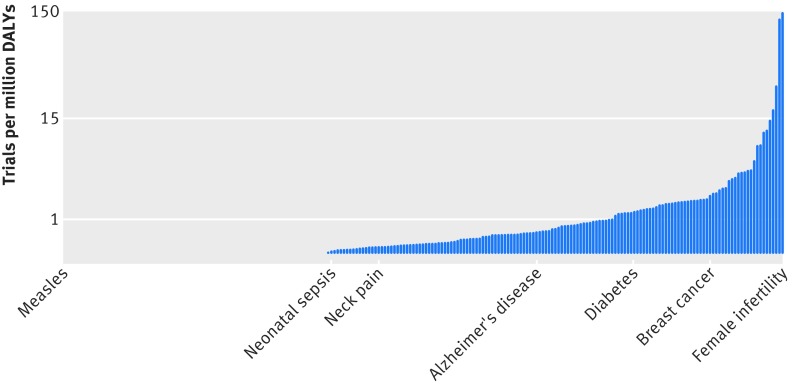
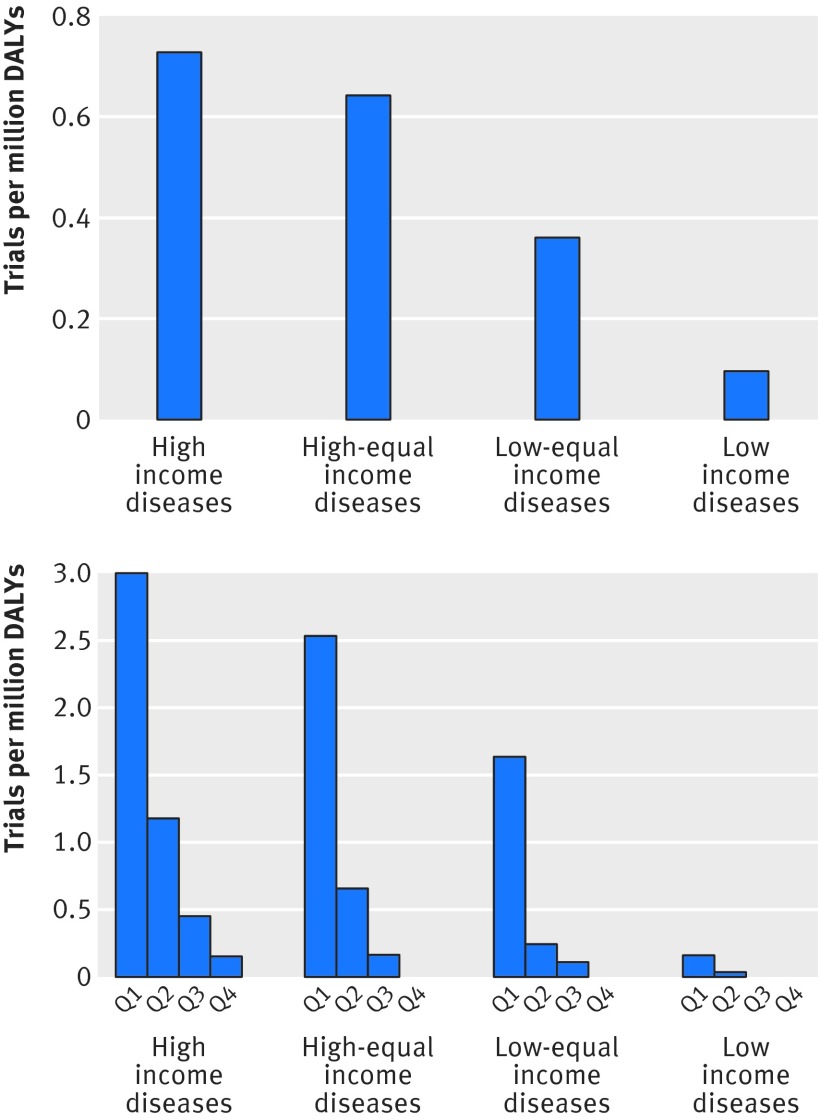
4190 abstracts were reviewed and 1351 primary randomised trials identified, of which 1097 could be classified using the global burden of disease taxonomy. Total disability adjusted life years was poorly associated with number of randomised trials and number of participants randomised in univariable analysis (Spearman's r=0.35 and 0.33, respectively), although it was a significant predictor in the univariable and multivariable models (P<0.001). Diseases for which the burden was predominantly located in low income regions had sevenfold fewer trials per million disability adjusted life years than diseases predominantly located in high income regions. However, only 26% of the variation in number of trials among diseases could be explained by total disability adjusted life years and the ratio of disability adjusted life years in low income regions to high income regions. Many high income type diseases (for example, neck pain, glomerulonephritis) have proportionally fewer randomised trials compared with low income type diseases (for example, vitamin A deficiency).
Overall, a weak association existed between global burden of disease and number of published randomised trials. A global observatory for research is needed to monitor and reduce the discordance between the output of randomised trials and global burden of disease.
确定发表的随机对照试验数量与全球疾病负担之间是否存在关联,某些疾病相对于其负担是否研究不足,以及随机试验的产出与全球疾病负担之间的关系是否可以用高收入和低收入地区的相对疾病负担来解释。
横断面调查。
2012 年 12 月发表并于 2013 年 11 月 17 日前在 PubMed 中索引的所有随机试验的主要报告。
239 种不同疾病或损伤的试验数量和随机分组人数;使用多变量回归,用总伤残调整生命年(衡量每种疾病的总体负担)和低收入与高收入地区伤残调整生命年比值(衡量疾病是否更可能影响高收入地区的人)来解释每种结果的差异。
共回顾了 4190 篇摘要,确定了 1351 项主要的随机试验,其中 1097 项可使用全球疾病负担分类进行分类。在单变量分析中,伤残调整生命年总计数与随机试验数量和随机分组人数的相关性较差(Spearman's r 分别为 0.35 和 0.33),但在单变量和多变量模型中是显著的预测因素(P<0.001)。负担主要在低收入地区的疾病每百万伤残调整生命年的试验数量比负担主要在高收入地区的疾病少 7 倍。然而,疾病之间试验数量的变化只有 26%可以用伤残调整生命年总计数和低收入地区与高收入地区伤残调整生命年比值来解释。许多高收入类型疾病(例如,颈部疼痛、肾小球肾炎)与低收入类型疾病(例如,维生素 A 缺乏症)相比,随机试验的比例相对较少。
总体而言,全球疾病负担与发表的随机试验数量之间存在弱关联。需要建立一个全球研究观察站来监测和减少随机试验的产出与全球疾病负担之间的不匹配。