Jepsen Rikke M H G, Spanager Lene, Lyk-Jensen Helle T, Dieckmann Peter, Østergaard Doris
Danish Institute for Medical Simulation (DIMS), Capital Region of Denmark and University of Copenhagen, Denmark.
Int J Med Educ. 2015 Feb 22;6:17-25. doi: 10.5116/ijme.54be.8f08.
The objectives of the study were to identify Danish anaesthesiologists' non-technical skills and to customise the Scottish-developed Anaesthetists' Non-Technical Skills instrument for Danish anaesthesiologists.
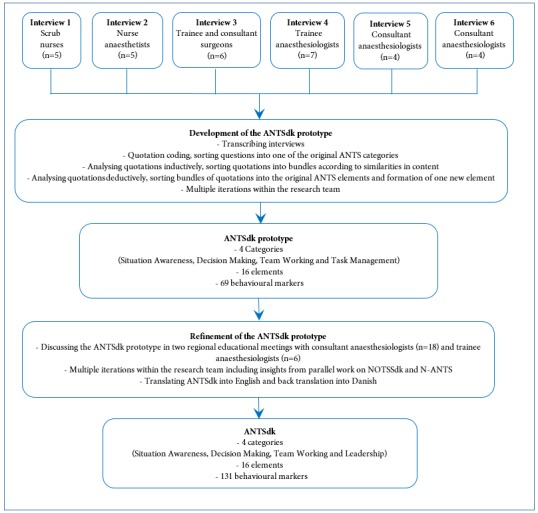
Six semi-structured group interviews were conducted with 31 operating room team members: anaes-thesiologists, nurse anaesthetists, surgeons, and scrub nurses. Interviews were transcribed verbatim and analysed using directed content analysis. Anaesthesiologists' non-technical skills were identified, coded, and sorted using the original instrument as a basis. The resulting prototype instrument was discussed with anaesthesiologists from 17 centres to ensure face validity.
Interviews lasted 46-67 minutes. Identified examples of anaesthesiologists' good or poor non-technical skills fit the four categories in the original instrument: situation awareness; decision making; team working; and task management. Anaesthesiologists' leadership role in the operating room was emphasised: the original 'Task Management' category was named 'Leadership'. One new element, 'Demonstrating self-awareness' was added under the category 'Situation Awareness'. Compared with the original instrument, half of the behavioural markers were new, which reflected that being aware of and communicating one's own abilities to the team; working systematically; and speaking up to avoid adverse events were important skills.
The Anaesthetists' Non-Technical Skills instrument was customised to a Danish setting using the identified non-technical skills for anaesthesiologists and the original instrument as basis. The customised instrument comprises four categories and 16 underpinning elements supported by multiple behavioural markers. Identifying non-technical skills through semi-structured group interviews and analysing them using direct content analysis proved a useful method for customising an assessment instrument to another setting.
本研究的目的是确定丹麦麻醉医生的非技术技能,并针对丹麦麻醉医生对苏格兰开发的《麻醉医生非技术技能》工具进行定制。
对31名手术室团队成员进行了6次半结构化小组访谈,这些成员包括麻醉医生、麻醉护士、外科医生和洗手护士。访谈内容逐字记录,并采用定向内容分析法进行分析。以原始工具为基础,对麻醉医生的非技术技能进行识别、编码和分类。与来自17个中心的麻醉医生讨论了生成的原型工具,以确保表面效度。
访谈持续了46 - 67分钟。所确定的麻醉医生非技术技能的良好或不良示例符合原始工具中的四个类别:态势感知;决策;团队协作;任务管理。强调了麻醉医生在手术室中的领导作用:将原始的“任务管理”类别命名为“领导能力”。在“态势感知”类别下增加了一个新元素“展现自我意识”。与原始工具相比,一半的行为指标是新的,这反映出向团队意识到并传达自己的能力、系统地工作以及直言以避免不良事件是重要技能。
以确定的麻醉医生非技术技能和原始工具为基础,将《麻醉医生非技术技能》工具定制为适用于丹麦的情况。定制后的工具包括四个类别和16个支撑要素,并由多个行为指标支持。通过半结构化小组访谈识别非技术技能并使用定向内容分析法进行分析,证明是将评估工具定制到另一种情况的有用方法。