Graziani Giorgio, Podestà Manuel A, Cucchiari David, Reggiani Francesco, Ponticelli Claudio
Nephrology and Dialysis Unit , Humanitas Clinical and Research Center , Rozzano, Milano , Italy.
Clin Kidney J. 2014 Aug;7(4):339-43. doi: 10.1093/ckj/sfu068. Epub 2014 Jul 15.
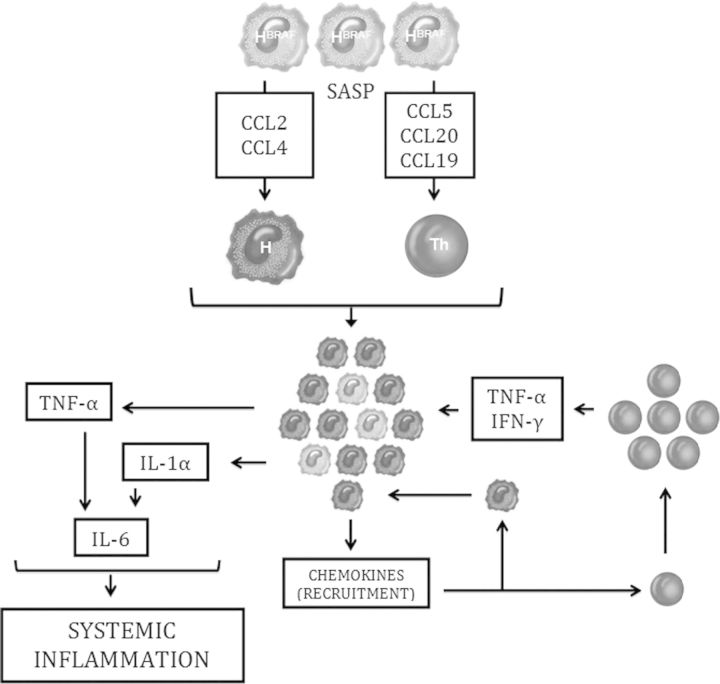
Erdheim-Chester disease (ECD) is a life-threatening multi-systemic non-Langerhans histiocytosis with cardiovascular complications as the leading cause of death. ECD affects the kidneys in up to 30% of cases, with fibrotic tissue deposition in the perirenal fat and renal hilum. Diagnosis is usually based on histological analysis of the pathologic tissue, which typically shows xanthogranulomatous infiltrates of foamy CD68+/CD1a- histiocytes surrounded by fibrosis. A consistent percentage of patients affected by ECD develop renal failure and hypertension as a consequence of renal artery stenosis and hydronephrosis. These conditions have been generally treated with the placement of stents and nephrostomies that frequently led to disappointing outcomes. Before the introduction of interferon-alpha (IFNα) treatment, the mortality rate was as high as 57% in the long term. Recent studies have granted new insights into the pathogenesis of ECD, which seems to bear a dual component of clonal and inflammatory disease. These advances led to use specific therapies targeting either the oncogenes (BRAF(V600E)) or the effectors of the immune response implicated in ECD (IL-1, TNFα). Drugs such as anakinra (recombinant human IL-1 receptor antagonist), infliximab (monoclonal antibody against TNFα) and vemurafenib (inhibitor of mutant BRAF) showed promising results in small single-centre series. Although larger trials will be needed to address the impact of these drugs on ECD prognosis and to select the most effective treatment, targeted therapies hold the premises to drastically change the outcome of this condition.
厄德里希-切斯特病(ECD)是一种危及生命的多系统非朗格汉斯组织细胞增多症,心血管并发症是主要死因。ECD在高达30%的病例中累及肾脏,肾周脂肪和肾门有纤维化组织沉积。诊断通常基于病理组织的组织学分析,其典型表现为泡沫状CD68+/CD1a-组织细胞的黄色肉芽肿性浸润,并伴有纤维化。一定比例的ECD患者会因肾动脉狭窄和肾积水而发展为肾衰竭和高血压。这些病症通常采用支架置入术和肾造瘘术治疗,但往往效果不佳。在引入干扰素-α(IFNα)治疗之前,长期死亡率高达57%。最近的研究为ECD的发病机制提供了新的见解,该病似乎具有克隆性疾病和炎性疾病的双重特征。这些进展促使人们使用针对致癌基因(BRAF(V600E))或参与ECD的免疫反应效应因子(IL-1、TNFα)的特异性疗法。阿那白滞素(重组人IL-1受体拮抗剂)、英夫利昔单抗(抗TNFα单克隆抗体)和维莫非尼(突变型BRAF抑制剂)等药物在小型单中心系列研究中显示出了有前景的结果。尽管需要更大规模的试验来评估这些药物对ECD预后的影响并选择最有效的治疗方法,但靶向治疗有望彻底改变这种疾病的预后。