Arsène Emmanuelle, Bleu Géraldine, Merlot Benjamin, Boulanger Loïc, Vinatier Denis, Kerdraon Olivier, Collinet Pierre
Department of Gynecology, Hospital Jeanne de Flandre, University Hospital of Lille, Lille, France.
Department of Gynecology, Hospital Jeanne de Flandre, University Hospital of Lille, Lille, France.; University of Lille-Nord-de-France, Lille, France.
J Gynecol Oncol. 2015 Apr;26(2):125-33. doi: 10.3802/jgo.2015.26.2.125.
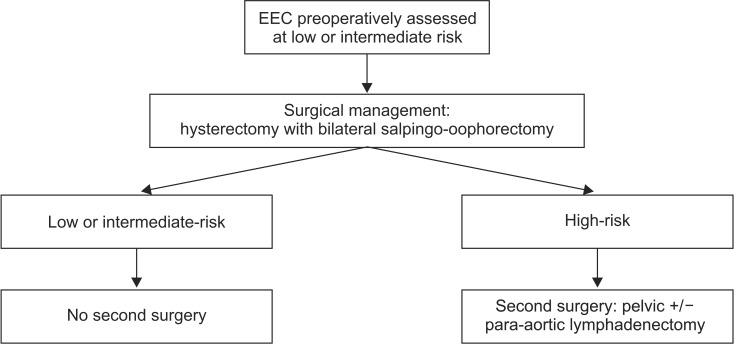
Since European Society for Medical Oncology (ESMO) recommendations and French guidelines, pelvic lymphadenectomy should not be systematically performed for women with early-stage endometrioid endometrial cancer (EEC) preoperatively assessed at presumed low- or intermediate-risk. The aim of our study was to evaluate the change of our surgical practices after ESMO recommendations, and to evaluate the rate and morbidity of second surgical procedure in case of understaging after the first surgery.
This retrospective single-center study included women with EEC preoperatively assessed at presumed low- or intermediate-risk who had surgery between 2006 and 2013. Two periods were defined the times before and after ESMO recommendations. Demographics characteristics, surgical management, operative morbidity, and rate of understaging were compared. The rate of second surgical procedure required for lymph node resection during the second period and its morbidity were also studied.
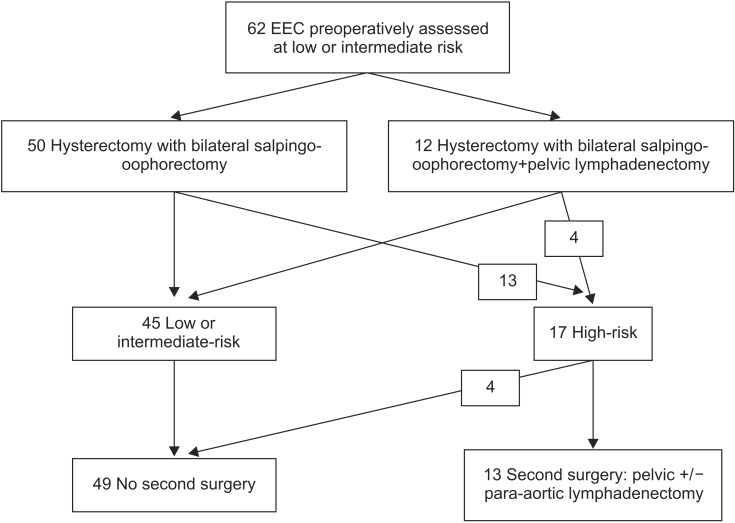
Sixty-one and sixty-two patients were operated for EEC preoperatively assessed at presumed low-or intermediate-risk before and after ESMO recommendations, respectively. Although immediate pelvic lymphadenectomy was performed more frequently during the first period than the second period (88.5% vs. 19.4%; p<0.001), the rate of postoperative risk-elevating or upstaging were comparable between the two periods (31.1% vs. 27.4%; p=0.71). Among the patients requiring second surgical procedure during the second period (21.0%), 30.8% did not undergo the second surgery due to their comorbidity or old age. For the patients who underwent second surgical procedure, mean operative time of the second procedure was 246.1±117.8 minutes. Third operation was required in 33.3% of them because of postoperative complications.
Since ESMO recommendations, second surgical procedure for lymph node resection is often required for women with EEC presumed at low- or intermediate-risk. This reoperation is not always performed due to age/comorbidity of the patients, and presents a significant morbidity.
自欧洲肿瘤内科学会(ESMO)发布相关建议及法国出台指南以来,对于术前评估为低风险或中风险的早期子宫内膜样子宫内膜癌(EEC)女性患者,不应常规进行盆腔淋巴结清扫术。我们研究的目的是评估ESMO建议发布后我们的手术方式的变化,并评估首次手术后分期不足时二次手术的发生率及并发症情况。
这项回顾性单中心研究纳入了2006年至2013年间接受手术的术前评估为低风险或中风险的EEC女性患者。定义了两个时期,即ESMO建议发布之前和之后的时间。比较了人口统计学特征、手术管理、手术并发症及分期不足的发生率。还研究了第二时期进行淋巴结切除所需的二次手术的发生率及其并发症情况。
分别有61例和62例术前评估为低风险或中风险的EEC患者在ESMO建议发布之前和之后接受了手术。尽管第一时期比第二时期更频繁地进行即时盆腔淋巴结清扫术(88.5%对19.4%;p<0.001),但两个时期术后风险升高或分期上调的发生率相当(31.1%对27.4%;p=0.71)。在第二时期需要二次手术的患者中(21.0%),30.8%由于合并症或年龄原因未接受二次手术。对于接受二次手术的患者,二次手术的平均手术时间为246.1±(117.8)分钟。其中33.3%的患者因术后并发症需要进行第三次手术。
自ESMO发布建议以来,对于术前评估为低风险或中风险的EEC女性患者,通常需要进行二次淋巴结切除手术。由于患者的年龄/合并症,这种再次手术并不总是能实施,且存在显著的并发症。