McCaffrey James, Coupes Beatrice, Chaloner Chris, Webb Nicholas J A, Barber Rachael, Lennon Rachel
Department of Paediatric Nephrology, Royal Manchester Children's Hospital, Central Manchester University Hospitals NHS Foundation Trust (CMFT), Manchester Academic Health Science Centre, Manchester, UK.
Pediatr Nephrol. 2015 Oct;30(10):1861-71. doi: 10.1007/s00467-015-3089-3. Epub 2015 Apr 15.
Critically ill children and neonates are at high risk of developing acute kidney injury (AKI). AKI is associated with short- and long-term renal impairment and increased mortality. Current methods of diagnosing AKI rely on measurements of serum creatinine, which is a late and insensitive marker. Few studies to date have assessed AKI biomarkers in a heterogeneous patient cohort.
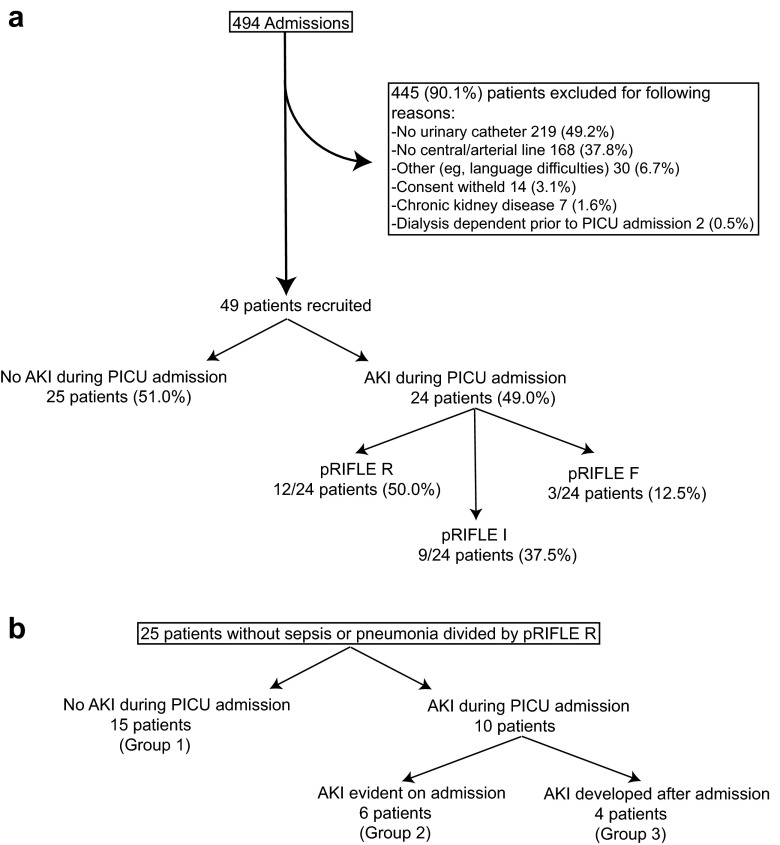
We conducted a prospective feasibility study in a paediatric intensive care setting over a 6-month period to describe the relationship between AKI (defined according to pRIFLE criteria) and new AKI biomarkers.
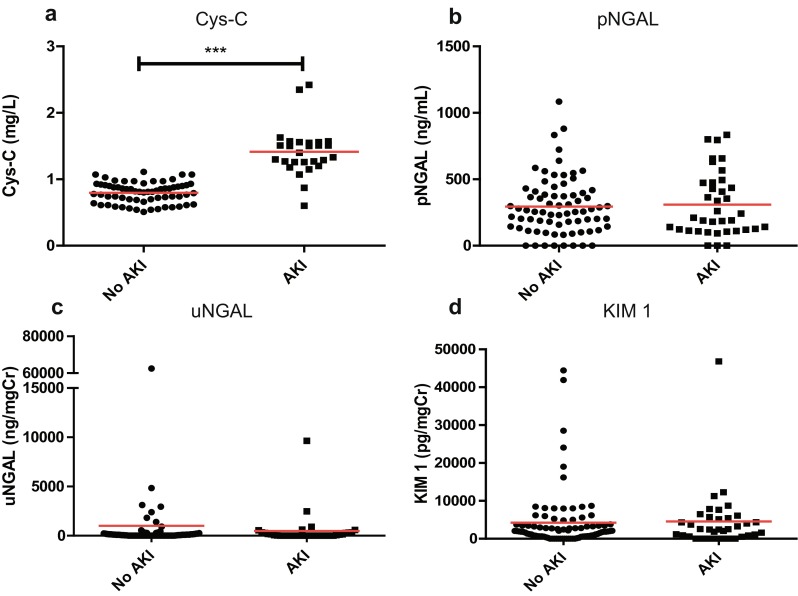
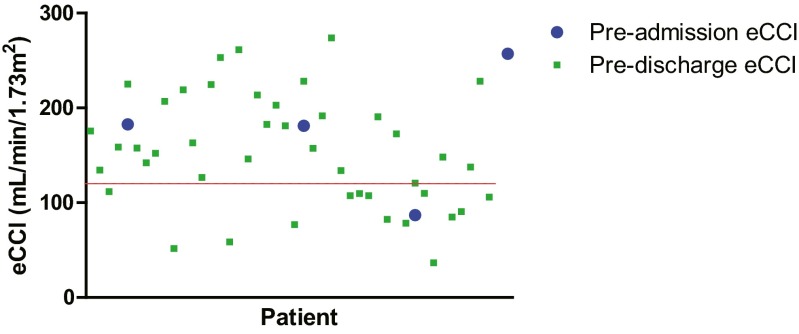
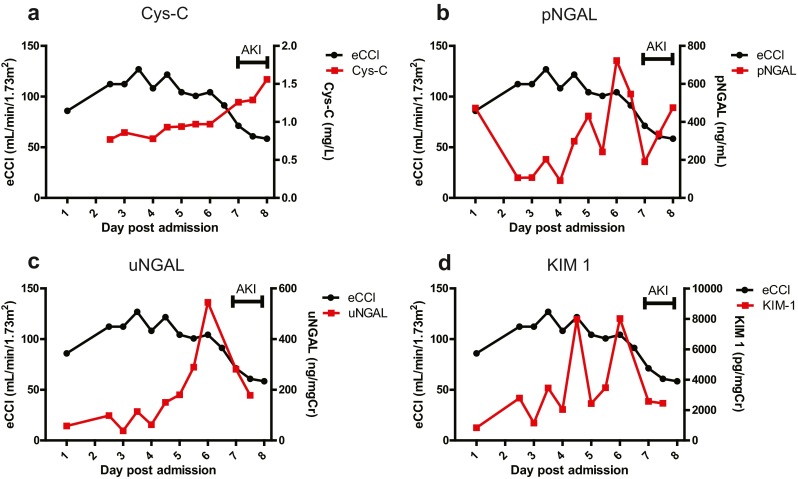
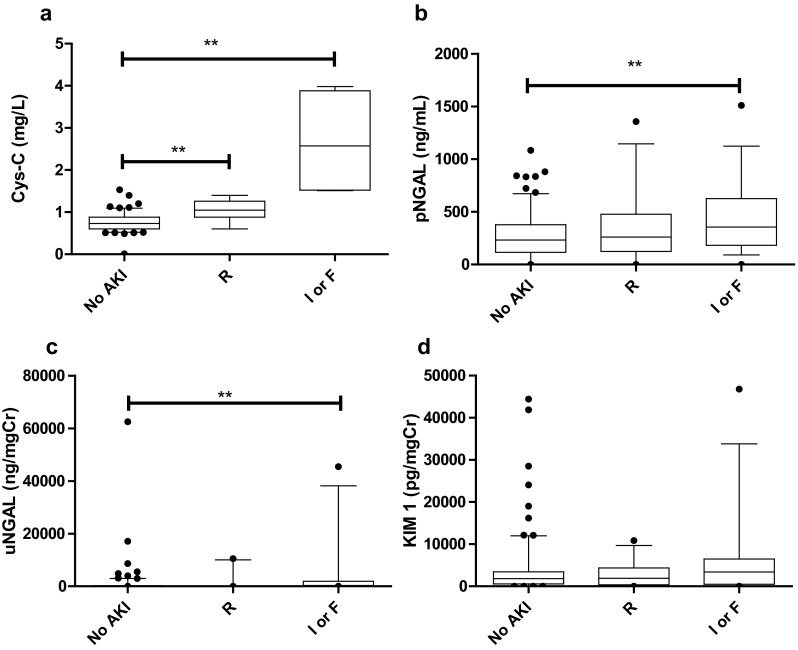
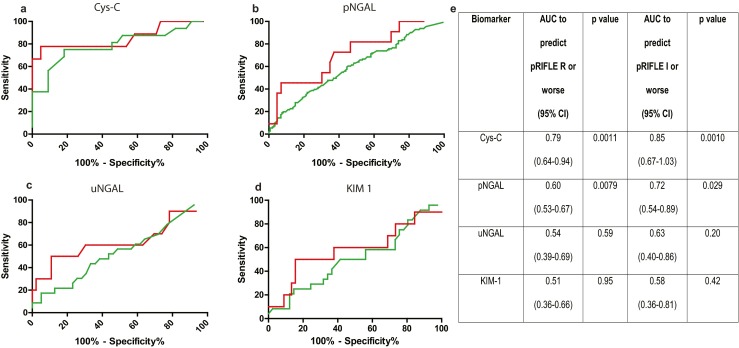
In total, 49 patients between the ages of 16 days and 15 years were recruited for measurement of plasma cystatin C (Cys-C) and neutrophil gelatinase-associated lipocalin (pNGAL) concentrations, as well as for urinary kidney injury molecule-1 (KIM-1) and urinary NGAL (uNGAL) concentrations. Almost one-half (49 %) of the patient cohort experienced an AKI episode, and Cys-C and pNGAL were the strongest candidates for the detection of AKI. Our data suggest that the widely used estimated baseline creatinine clearance value of 120 mL/min/1.73 m(2) underestimates actual baseline function in patients admitted to paediatric intensive care units.
This investigation demonstrates the feasibility of new AKI biomarker testing in a mixed patient cohort and provides novel biomarker profiling for further evaluation.
危重症儿童和新生儿发生急性肾损伤(AKI)的风险很高。AKI与短期和长期肾功能损害及死亡率增加相关。目前诊断AKI的方法依赖于血清肌酐测定,而血清肌酐是一种出现较晚且不敏感的标志物。迄今为止,很少有研究在异质性患者队列中评估AKI生物标志物。
我们在儿科重症监护病房进行了一项为期6个月的前瞻性可行性研究,以描述AKI(根据pRIFLE标准定义)与新的AKI生物标志物之间的关系。
总共招募了49名年龄在16天至15岁之间的患者,测量其血浆胱抑素C(Cys-C)和中性粒细胞明胶酶相关脂质运载蛋白(pNGAL)浓度,以及尿肾损伤分子-1(KIM-1)和尿NGAL(uNGAL)浓度。几乎一半(49%)的患者队列经历了AKI发作,Cys-C和pNGAL是检测AKI的最强候选标志物。我们的数据表明,广泛使用的估计基线肌酐清除率值120 mL/min/1.73 m²低估了入住儿科重症监护病房患者的实际基线功能。
本研究证明了在混合患者队列中进行新的AKI生物标志物检测的可行性,并为进一步评估提供了新的生物标志物概况。