Sánchez-González Javier, Fernandez-Jiménez Rodrigo, Nothnagel Nils D, López-Martín Gonzalo, Fuster Valentin, Ibañez Borja
Philips Healthcare Iberia, Maria de Portugal 1. 28050, Madrid, Spain.
Centro Nacional de Investigaciones Cardiovasculares (CNIC), Melchor Fernandez Almagro 3. 28029, Madrid, Spain.
J Cardiovasc Magn Reson. 2015 Feb 19;17(1):21. doi: 10.1186/s12968-015-0116-2.
In-vivo quantification of cardiac perfusion is of great research and clinical value. The dual-bolus strategy is universally used in clinical protocols but has known limitations. The dual-saturation acquisition strategy has been proposed as a more accurate alternative, but has not been validated across the wide range of perfusion rates encountered clinically. Dual-saturation acquisition also lacks a clinically-applicable procedure for optimizing parameter selection. Here we present a comprehensive validation study of dual-saturation strategy in vitro and in vivo.
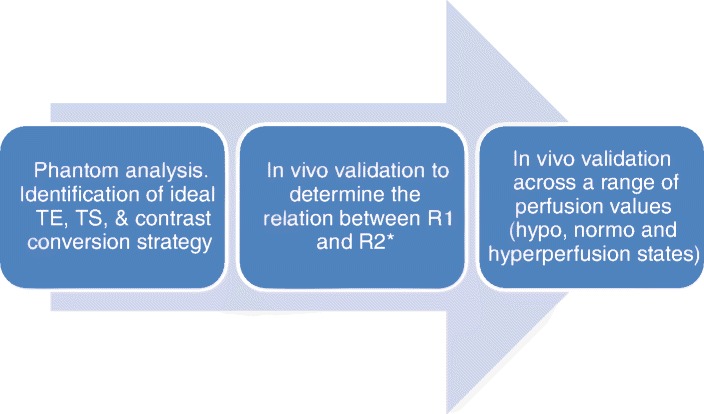
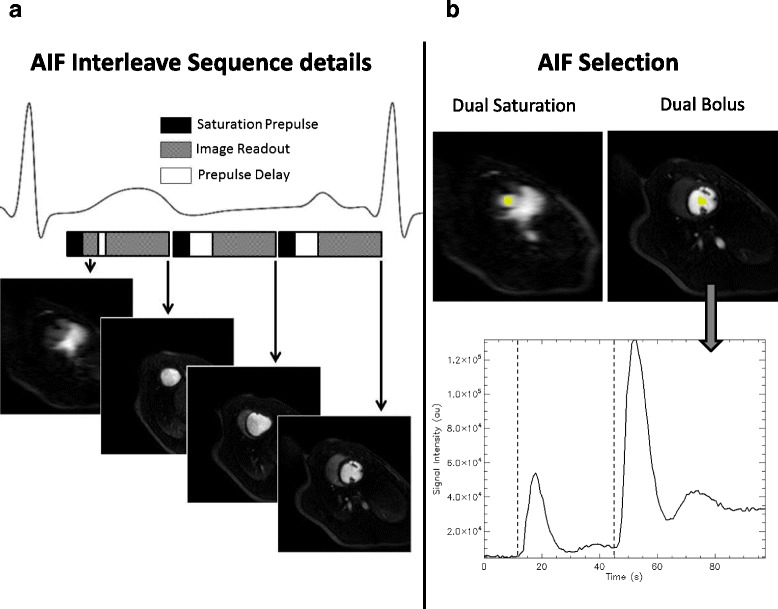
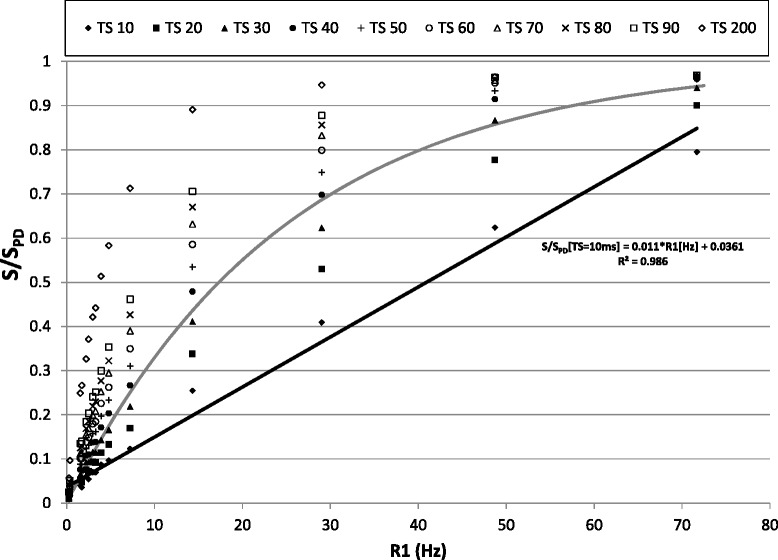
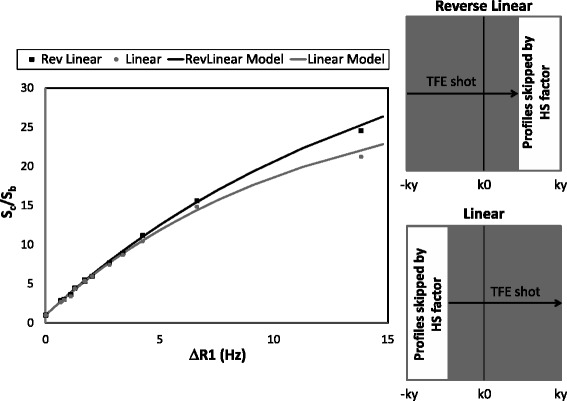
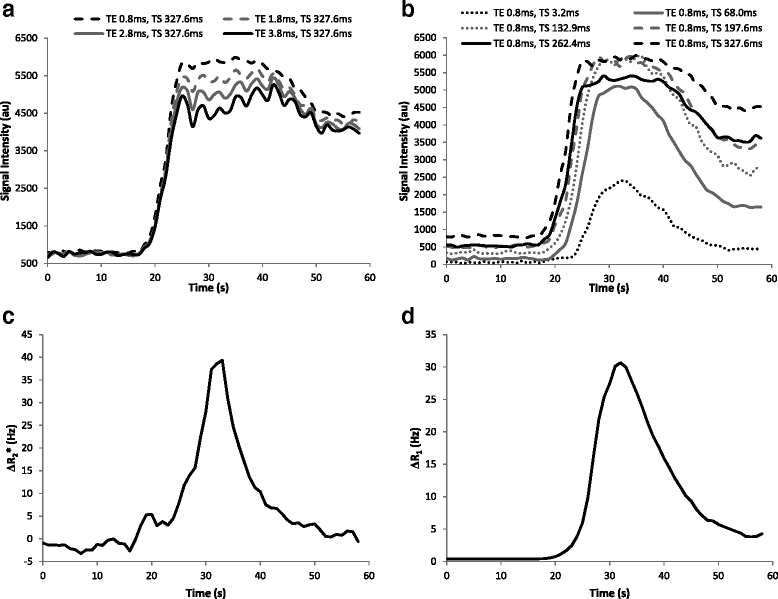
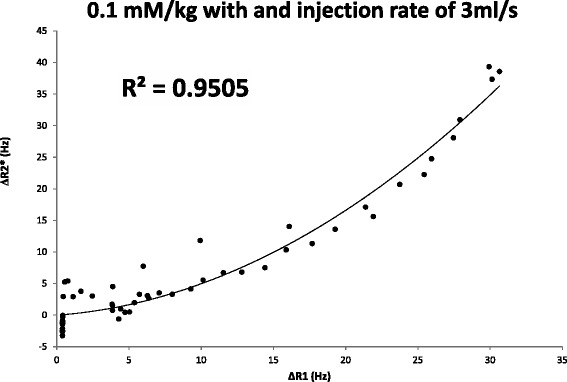
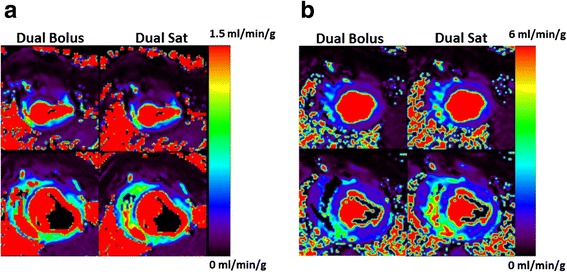
The impact of saturation time and profile ordering in acquisitions was systematically analyzed in a phantom consisting of 15 tubes containing different concentrations of contrast agent. In-vivo experiments in healthy pigs were conducted to evaluate the effect of R2* on the definition of the arterial input function (AIF) and to evaluate the relationship between R2* and R1 variations during first-pass of the contrast agent. Quantification by dual-saturation perfusion was compared with the reference-standard dual-bolus strategy in 11 pigs with different grades of myocardial perfusion.
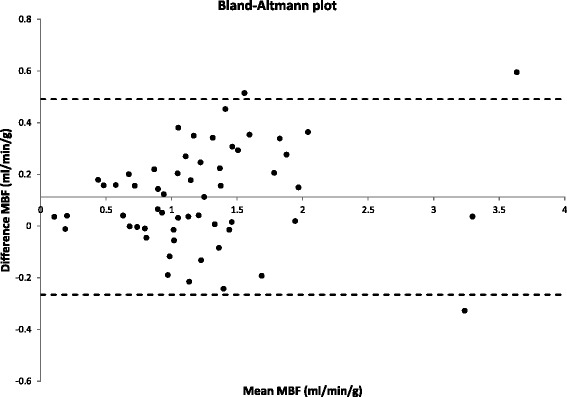
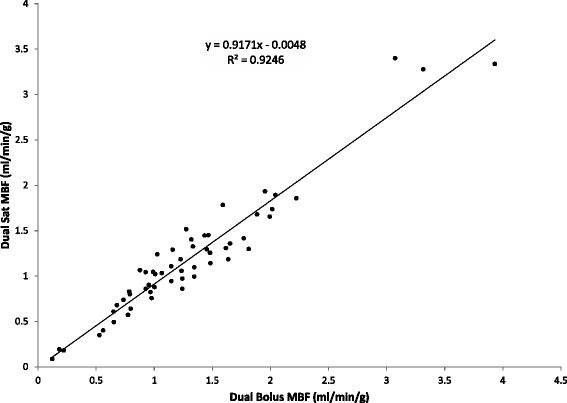
Adequate flow estimation by the dual-saturation strategy is achieved with myocardial tissue saturation times around 100 ms (always <30 ms of AIF), with the lowest echo time, and following a signal model for contrast conversion that takes into account the residual R2* effect and profile ordering. There was a good correlation and agreement between myocardial perfusion quantitation by dual-saturation and dual-bolus techniques (R(2) = 0.92, mean difference of 0.1 ml/min/g; myocardial perfusion ranges between 0.18 and 3.93 ml/min/g).
The dual-saturation acquisition strategy produces accurate estimates of absolute myocardial perfusion in vivo. The procedure presented here can be applied with minimal interference in standard clinical procedures.
心脏灌注的体内定量具有重大的研究和临床价值。双团注策略在临床方案中被广泛使用,但存在已知的局限性。双饱和采集策略已被提出作为一种更准确的替代方法,但尚未在临床遇到的广泛灌注率范围内得到验证。双饱和采集也缺乏一种临床适用的程序来优化参数选择。在此,我们展示了一项双饱和策略在体外和体内的全面验证研究。
在一个由15根装有不同浓度造影剂的试管组成的模型中,系统地分析了采集过程中饱和时间和轮廓排序的影响。在健康猪身上进行体内实验,以评估R2对动脉输入函数(AIF)定义的影响,并评估造影剂首过期间R2与R1变化之间的关系。在11只具有不同程度心肌灌注的猪中,将双饱和灌注定量与参考标准双团注策略进行比较。
通过双饱和策略实现了足够的血流估计,心肌组织饱和时间约为100毫秒(始终<AIF的30毫秒),采用最低回波时间,并遵循一种考虑残余R2*效应和轮廓排序的造影剂转换信号模型。双饱和技术和双团注技术对心肌灌注的定量之间存在良好的相关性和一致性(R(2)=0.92,平均差异为0.1毫升/分钟/克;心肌灌注范围在0.18至3.93毫升/分钟/克之间)。
双饱和采集策略可在体内准确估计绝对心肌灌注。此处介绍的程序在标准临床程序中的干扰最小。