Ho Thai H, Liu Xian-De, Huang Yanqing, Warneke Carla L, Johnson Marcella M, Hoang Anh, Tamboli Pheroze, Wang Fen, Jonasch Eric
Division of Hematology and Medical Oncology, Mayo Clinic, Scottsdale, USA.
Department of Genitourinary Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, USA.
BMC Cancer. 2015 Apr 18;15:304. doi: 10.1186/s12885-015-1302-1.
Angiogenesis plays a role in tumor growth and is partly mediated by factors in both the fibroblast growth factor (FGF) and vascular endothelial growth factor (VEGF) pathways. Durable clinical responses with VEGF tyrosine kinase inhibitors (TKIs) may be limited by intrinsic tumor resistance. We hypothesized that FGF signaling may impact clinical responses to sorafenib.
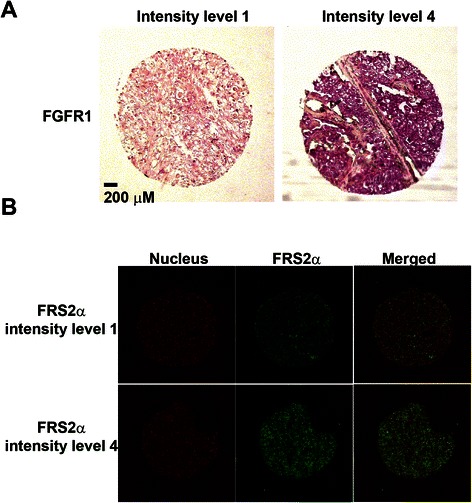
Nephrectomy material was available from 40 patients with metastatic renal cell carcinoma (RCC) enrolled in a phase II clinical trial of sorafenib ± interferon (ClinicalTrials.gov Identifier NCT00126594). Fibroblast growth factor receptor 1 (FGFR1) and fibroblast growth factor receptor substrate 2 alpha (FRS2α) expression was assessed by in situ hybridization and immunofluorescence, respectively. The relationship between fibroblast growth factor pathway marker levels and progression-free survival (PFS) was analyzed using Kaplan-Meier and Cox proportional hazards regression methods.
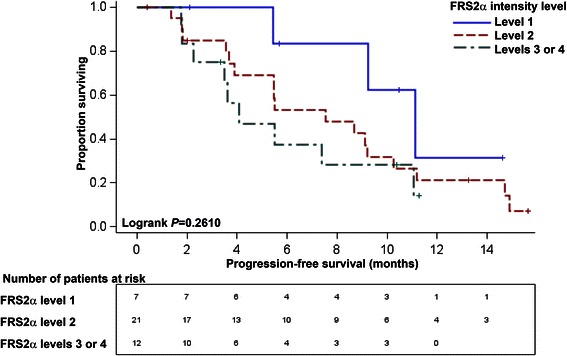
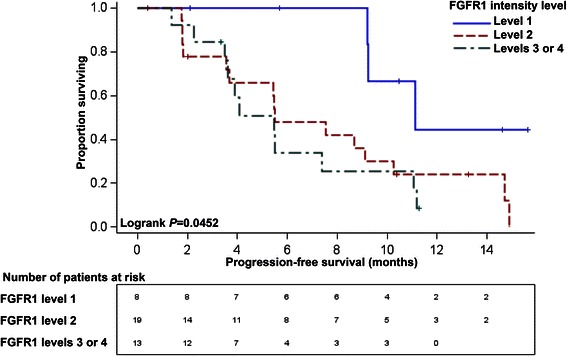
Univariate analysis indicated that more intense FGFR1 staining was associated with shorter PFS (log-rank P = 0.0452), but FRS2α staining was not significantly associated with PFS (log-rank P = 0.2610). Multivariate Cox proportional hazards regression models were constructed for FGFR1 and FRS2α individually, adjusting for baseline Eastern Cooperative Oncology Group performance status, treatment arm and anemia status. When adjusted for each of these variables, the highest intensity level of FGFR1 (level 3 or 4) had increased progression risk relative to the lowest intensity level of FGFR1 (level 1) (P = 0.0115). The highest intensity level of FRS2α (level 3 or 4) had increased progression risk relative to the lowest intensity level of FRS2α (level 1) (P = 0.0126).
Increased expression of FGFR1 and FRS2α was associated with decreased PFS among patients with metastatic RCC treated with sorafenib. The results suggest that FGF pathway activation may impact intrinsic resistance to VEGF receptor inhibition.
血管生成在肿瘤生长中起作用,部分由成纤维细胞生长因子(FGF)和血管内皮生长因子(VEGF)途径中的因子介导。VEGF酪氨酸激酶抑制剂(TKIs)的持久临床反应可能受到肿瘤内在抗性的限制。我们假设FGF信号传导可能影响对索拉非尼的临床反应。
肾切除术材料来自40例参加索拉非尼±干扰素II期临床试验的转移性肾细胞癌(RCC)患者(ClinicalTrials.gov标识符NCT00126594)。分别通过原位杂交和免疫荧光评估成纤维细胞生长因子受体1(FGFR1)和成纤维细胞生长因子受体底物2α(FRS2α)的表达。使用Kaplan-Meier和Cox比例风险回归方法分析成纤维细胞生长因子途径标志物水平与无进展生存期(PFS)之间的关系。
单因素分析表明,FGFR1染色强度越高,PFS越短(对数秩P = 0.0452),但FRS2α染色与PFS无显著相关性(对数秩P = 0.2610)。分别针对FGFR1和FRS2α构建多变量Cox比例风险回归模型,调整基线东部肿瘤协作组(ECOG)体能状态、治疗组和贫血状态。当对这些变量中的每一个进行调整时,相对于FGFR1的最低强度水平(1级),FGFR1的最高强度水平(3级或4级)具有增加的进展风险(P = 0.0115)。相对于FRS2α的最低强度水平(1级),FRS2α的最高强度水平(3级或4级)具有增加的进展风险(P = 0.0126)。
在接受索拉非尼治疗的转移性RCC患者中,FGFR1和FRS2α表达增加与PFS降低相关。结果表明,FGF途径激活可能影响对VEGF受体抑制的内在抗性。