Gattarello Simone, Ramírez Sergio, Almarales José Rafael, Borgatta Bárbara, Lagunes Leonel, Encina Belén, Rello Jordi
Servicio de Medicina Intensiva, Institut de Recerca Vall d'Hebron (VHIR); Hospital Universitario Vall d'Hebron, Departamento de Medicina, Universidad Autónoma de Barcelona, Barcelona, España.
Servicio de Medicina Intensiva, Clínica Comfamiliar, Universidad Tecnológica de Pereira, Risaralda, Colombia.
Rev Bras Ter Intensiva. 2015 Jan-Mar;27(1):44-50. doi: 10.5935/0103-507X.20150008. Epub 2015 Mar 1.
To assess the adherence to Infectious Disease Society of America/American Thoracic Society guidelines and the causes of lack of adherence during empirical antibiotic prescription in severe pneumonia in Latin America.
A clinical questionnaire was submitted to 36 physicians from Latin America; they were asked to indicate the empirical treatment in two fictitious cases of severe respiratory infection: community-acquired pneumonia and nosocomial pneumonia.
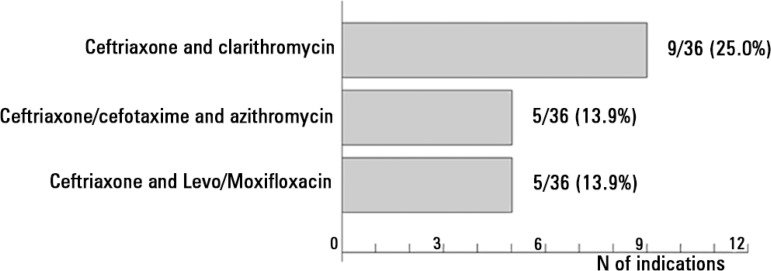
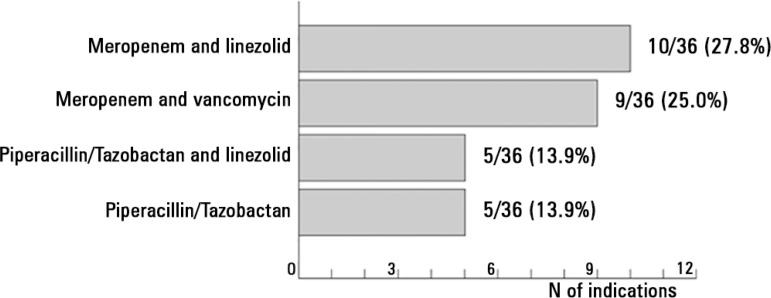
In the case of community acquired pneumonia, 11 prescriptions of 36 (30.6%) were compliant with international guidelines. The causes for non-compliant treatment were monotherapy (16.0%), the unnecessary prescription of broad-spectrum antibiotics (40.0%) and the use of non-recommended antibiotics (44.0%). In the case of nosocomial pneumonia, the rate of adherence to the Infectious Disease Society of America/American Thoracic Society guidelines was 2.8% (1 patient of 36). The reasons for lack of compliance were monotherapy (14.3%) and a lack of dual antibiotic coverage against Pseudomonas aeruginosa (85.7%). If monotherapy with an antipseudomonal antibiotic was considered adequate, the antibiotic treatment would be adequate in 100% of the total prescriptions.
The compliance rate with the Infectious Disease Society of America/American Thoracic Society guidelines in the community-acquired pneumonia scenario was 30.6%; the most frequent cause of lack of compliance was the indication of monotherapy. In the case of nosocomial pneumonia, the compliance rate with the guidelines was 2.8%, and the most important cause of non-adherence was lack of combined antipseudomonal therapy. If the use of monotherapy with an antipseudomonal antibiotic was considered the correct option, the treatment would be adequate in 100% of the prescriptions.
评估拉丁美洲地区在重症肺炎经验性抗生素处方过程中对美国传染病学会/美国胸科学会指南的遵循情况以及未遵循的原因。
向36名来自拉丁美洲的医生发放了一份临床调查问卷;要求他们指出在两例虚构的严重呼吸道感染病例(社区获得性肺炎和医院获得性肺炎)中的经验性治疗方案。
在社区获得性肺炎病例中,36份处方中有11份(30.6%)符合国际指南。治疗不依从的原因包括单一疗法(16.0%)、不必要地开具广谱抗生素(40.0%)以及使用未推荐的抗生素(44.0%)。在医院获得性肺炎病例中,遵循美国传染病学会/美国胸科学会指南的比例为2.8%(36例中有1例)。不依从的原因包括单一疗法(14.3%)以及缺乏针对铜绿假单胞菌的双联抗生素覆盖(85.7%)。如果认为使用抗假单胞菌抗生素进行单一疗法是足够的,那么在所有处方中100%的抗生素治疗将是足够的。
在社区获得性肺炎情况下,遵循美国传染病学会/美国胸科学会指南的比例为30.6%;最常见的不遵循原因是单一疗法的使用。在医院获得性肺炎病例中,遵循指南的比例为2.8%,最重要的不依从原因是缺乏联合抗假单胞菌治疗。如果将使用抗假单胞菌抗生素进行单一疗法视为正确选择,那么在100%的处方中治疗将是足够的。