Nkoke Clovis, Kuate Liliane Mfeukeu, Luchuo Engelbert Bain, Edie Sandrine Dikosso, Boombhi Jerome, Menanga Alain
Faculty of Medicine and Biomedical Sciences, University of Yaounde I, Yaounde, Cameroon.
Cardiology Unit, Yaounde Central Hospital, Yaounde, Cameroon.
BMC Res Notes. 2015 Apr 28;8:168. doi: 10.1186/s13104-015-1140-x.
Sub-Saharan Africa is undergoing epidemiological transition with an increase in the prevalence of cardiovascular diseases that will add to the already devastating burden of infectious diseases such as human immunodeficiency virus infection. Human immunodeficiency virus infection is increasingly being recognized as an important etiological factor for dilated cardiomyopathy with the potential complication of intraventricular thrombus. However, biventricular thrombi are extremely rare. We report on a rare finding of biventricular thrombi in dilated cardiomyopathy in a patient with human immunodeficiency virus infection in Cameroon.
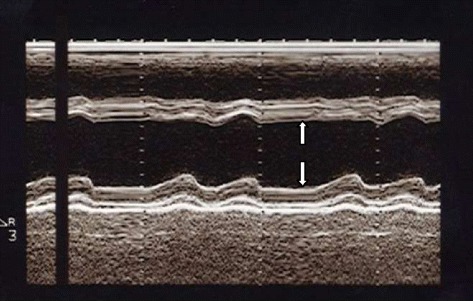
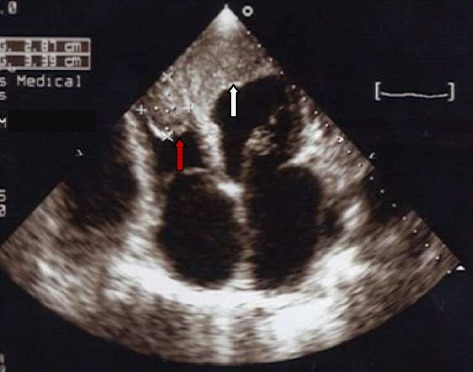
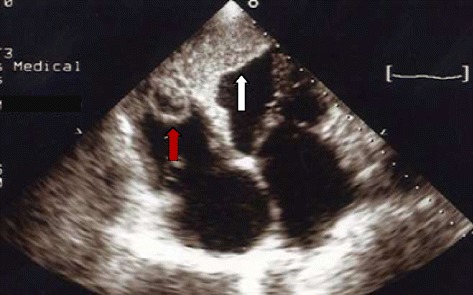
A 52-year old Cameroonian male patient with human immunodeficiency virus infection since 4 years, longstanding heavy alcohol consumption and cigarette smoking presented with gradually worsening shortness of breath, fatigue, persistent dry cough and lower extremity swelling of about two weeks duration. Congestive heart failure was diagnosed. Echocardiography showed left ventricular chamber enlargement with severe left ventricular systolic dysfunction and biventricular thrombi. The thrombi were immobile and regular in configuration, suggesting they were old. He was treated with a conventional heart failure treatment including loop diuretics and angiotensin converting enzyme inhibitors and anticoagulants for the biventricular thrombi. Six months later, a control echocardiography showed a significant decrease in the size of the thrombi. There was no evidence of systemic or pulmonary embolization during follow up.
Dilated cardiomyopathy may be seen in patients with human immunodeficiency virus infection, although other mechanisms needs to be assessed, but the occurrence of biventricular thrombi is rare.
撒哈拉以南非洲正在经历流行病学转变,心血管疾病患病率上升,这将加重诸如人类免疫缺陷病毒感染等传染病已有的沉重负担。人类免疫缺陷病毒感染日益被认为是扩张型心肌病的一个重要病因,可能并发心室内血栓形成。然而,双心室血栓极为罕见。我们报告在喀麦隆一名感染人类免疫缺陷病毒的患者中,在扩张型心肌病中发现罕见的双心室血栓。
一名52岁的喀麦隆男性患者,4年前感染人类免疫缺陷病毒,长期大量饮酒和吸烟,出现逐渐加重的呼吸急促、疲劳、持续干咳和下肢肿胀约两周。诊断为充血性心力衰竭。超声心动图显示左心室腔扩大,伴有严重的左心室收缩功能障碍和双心室血栓。血栓固定不动,形态规则,提示为陈旧性血栓。他接受了包括袢利尿剂、血管紧张素转换酶抑制剂和针对双心室血栓的抗凝剂在内的传统心力衰竭治疗。6个月后,对照超声心动图显示血栓大小显著减小。随访期间未发现全身或肺栓塞的证据。
尽管需要评估其他机制,但人类免疫缺陷病毒感染患者可能会出现扩张型心肌病,而双心室血栓的发生较为罕见。