Balzer Felix, Weiß Björn, Kumpf Oliver, Treskatsch Sascha, Spies Claudia, Wernecke Klaus-Dieter, Krannich Alexander, Kastrup Marc
Department of Anaesthesiology and Intensive Care Medicine, Charité - Universitätsmedizin Berlin, Charitéplatz 1, Berlin, 10117, Germany.
Charité - Universitätsmedizin Berlin and SOSTANA GmbH, Wildensteiner Straße 27, Berlin, 10318, Germany.
Crit Care. 2015 Apr 28;19(1):197. doi: 10.1186/s13054-015-0929-2.
There is increasing evidence that deep sedation is detrimental to critically ill patients. The aim of this study was to examine effects of deep sedation during the early period after ICU admission on short- and long-term survival.
In this observational, matched-pair analysis, patients receiving mechanical ventilation that were admitted to ICUs of a tertiary university hospital in six consecutive years were grouped as either lightly or deeply sedated within the first 48 hours after ICU admission. The Richmond Agitation-Sedation Score (RASS) was used to assess sedation depth (light sedation: -2 to 0; deep: -3 or below). Multivariate Cox regression was conducted to investigate the impact of early deep sedation within the first 48 hours of admission on in-hospital and two-year follow-up survival.
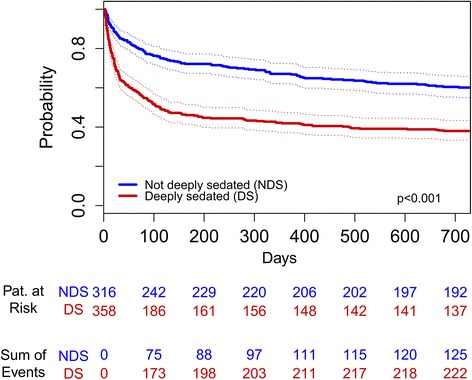
In total, 1,884 patients met inclusion criteria out of which 27.2% (n = 513) were deeply sedated. Deeply sedated patients had longer ventilation times, increased length of stay and higher rates of mortality. Early deep sedation was associated with a hazard ratio of 1.661 (95% CI: 1.074 to 2.567; P = 0.022) for in-hospital survival and 1.866 (95% CI: 1.351 to 2.576; P < 0.001) for two-year follow-up survival.
Early deep sedation during the first 48 hours of intensive care treatment was associated with decreased in-hospital and two-year follow-up survival. Since early deep sedation is a modifiable risk factor, this data shows an urgent need for prospective clinical trials focusing on light sedation in the early phase of ICU treatment.
越来越多的证据表明,深度镇静对重症患者有害。本研究的目的是探讨重症监护病房(ICU)入院早期深度镇静对短期和长期生存的影响。
在这项观察性配对分析中,连续六年入住一所三级大学医院ICU并接受机械通气的患者,在ICU入院后的前48小时内被分为浅镇静组或深镇静组。使用里士满躁动-镇静评分(RASS)评估镇静深度(浅镇静:-2至0;深镇静:-3或更低)。进行多变量Cox回归分析,以研究入院后48小时内早期深度镇静对住院期间和两年随访生存的影响。
共有1884例患者符合纳入标准,其中27.2%(n = 513)为深度镇静。深度镇静患者的通气时间更长,住院时间延长,死亡率更高。早期深度镇静与住院生存的风险比为1.661(95%置信区间:1.074至2.567;P = 0.022),两年随访生存的风险比为1.866(95%置信区间:1.351至2.576;P < 0.001)。
重症监护治疗的前48小时内早期深度镇静与住院期间及两年随访生存率降低有关。由于早期深度镇静是一个可改变的风险因素,该数据表明迫切需要开展前瞻性临床试验,重点关注ICU治疗早期的浅镇静。