Wing Simon, Rider Lisa G, Johnson Jay R, Miller Federick W, Matteson Eric L, Crowson Cynthia S, Gabriel Sherine E
The Johns Hopkins University, Laurel, Maryland, USA.
Environmental Autoimmunity Group, Clinical Research Branch, National Institute of Environmental Health Sciences, National Institutes of Health, Bethesda, Maryland, USA.
BMJ Open. 2015 May 15;5(5):e006636. doi: 10.1136/bmjopen-2014-006636.
To examine the influence of solar cycle and geomagnetic effects on the incidence of giant cell arteritis (GCA) and rheumatoid arthritis (RA).
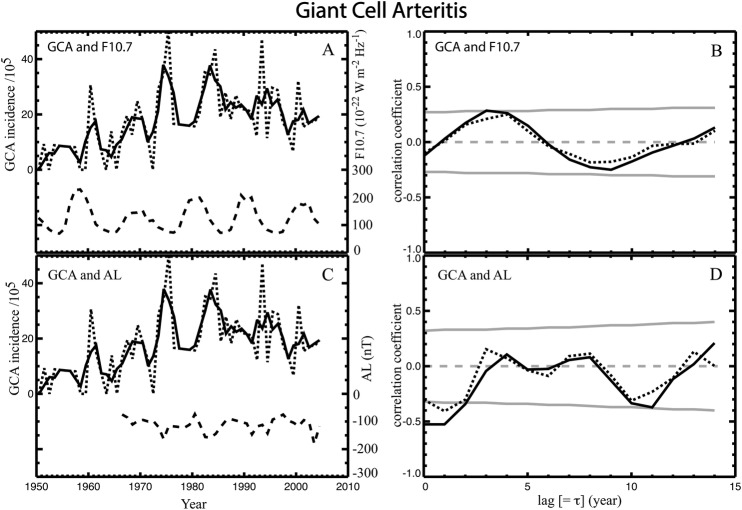
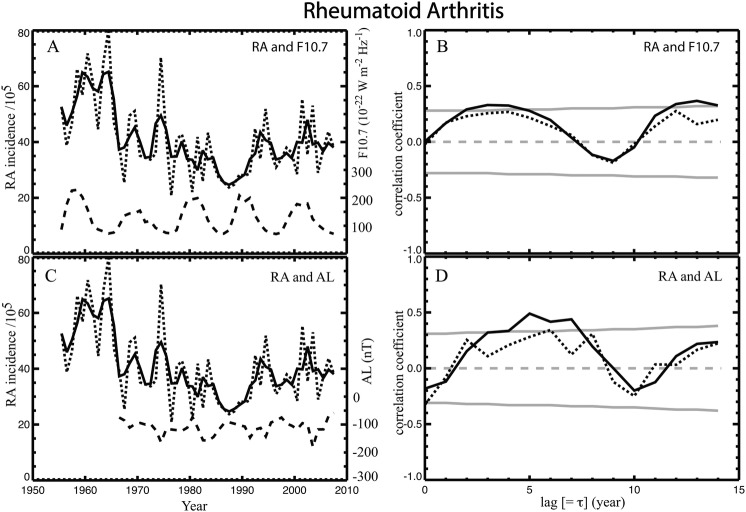
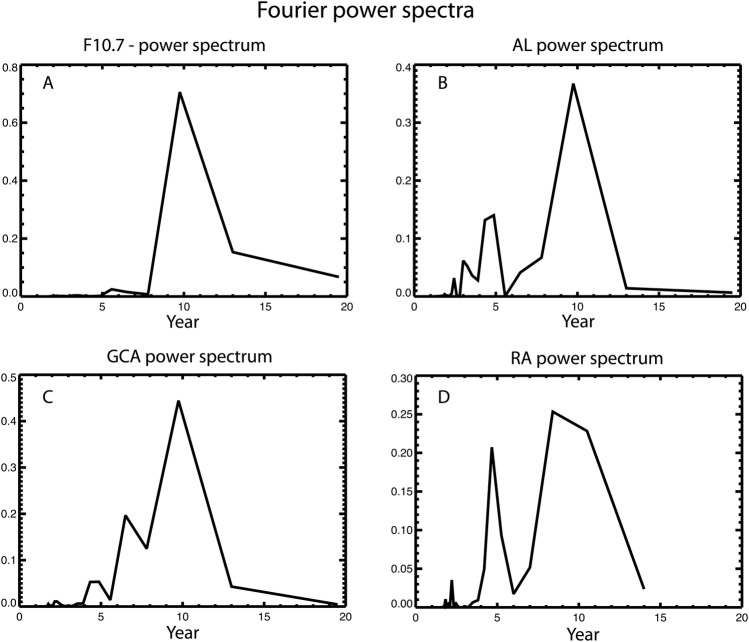
We used data from patients with GCA (1950-2004) and RA (1955-2007) obtained from population-based cohorts. Yearly trends in age-adjusted and sex-adjusted incidence were correlated with the F10.7 index (solar radiation at 10.7 cm wavelength, a proxy for the solar extreme ultraviolet radiation) and AL index (a proxy for the westward auroral electrojet and a measure of geomagnetic activity). Fourier analysis was performed on AL, F10.7, and GCA and RA incidence rates.
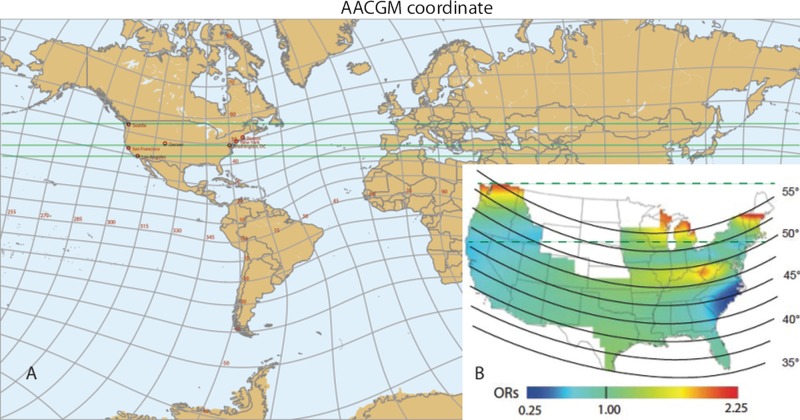
The correlation of GCA incidence with AL is highly significant: GCA incidence peaks 0-1 year after the AL reaches its minimum (ie, auroral electrojet reaches a maximum). The correlation of RA incidence with AL is also highly significant. RA incidence rates are lowest 5-7 years after AL reaches maximum. AL, GCA and RA incidence power spectra are similar: they have a main peak (periodicity) at about 10 years and a minor peak at 4-5 years. However, the RA incidence power spectrum main peak is broader (8-11 years), which partly explains the lower correlation between RA onset and AL. The auroral electrojets may be linked to the decline of RA incidence more strongly than the onset of RA. The incidences of RA and GCA are aligned in geomagnetic latitude.
AL and the incidences of GCA and RA all have a major periodicity of about 10 years and a secondary periodicity at 4-5 years. Geomagnetic activity may explain the temporal and spatial variations, including east-west skewness in geographic coordinates, in GCA and RA incidence, although the mechanism is unknown. The link with solar, geospace and atmospheric parameters need to be investigated. These novel findings warrant examination in other populations and with other autoimmune diseases.
研究太阳活动周期和地磁效应对巨细胞动脉炎(GCA)和类风湿关节炎(RA)发病率的影响。
我们使用了基于人群队列研究中GCA患者(1950 - 2004年)和RA患者(1955 - 2007年)的数据。年龄和性别调整后的年发病率趋势与F10.7指数(10.7厘米波长的太阳辐射,代表太阳极紫外辐射)和AL指数(代表向西极光电集流,是地磁活动的一种度量)相关。对AL、F10.7以及GCA和RA发病率进行了傅里叶分析。
GCA发病率与AL的相关性非常显著:在AL达到最小值(即极光电集流达到最大值)后的0 - 1年,GCA发病率达到峰值。RA发病率与AL的相关性也非常显著。在AL达到最大值后的5 - 7年,RA发病率最低。AL、GCA和RA发病率的功率谱相似:它们在约10年处有一个主峰(周期性),在4 - 5年处有一个次峰。然而,RA发病率功率谱的主峰更宽(8 - 11年),这部分解释了RA发病与AL之间较低的相关性。极光电集流与RA发病率下降的联系可能比与RA发病的联系更强。RA和GCA的发病率在地磁纬度上是一致的。
AL以及GCA和RA的发病率都有一个约10年的主要周期性和一个4 - 5年的次要周期性。地磁活动可能解释了GCA和RA发病率的时间和空间变化,包括地理坐标上的东西偏斜,尽管其机制尚不清楚。需要研究与太阳、地球空间和大气参数的联系。这些新发现值得在其他人群和其他自身免疫性疾病中进行检验。