Subak Leslee L, King Wendy C, Belle Steven H, Chen Jia-Yuh, Courcoulas Anita P, Ebel Faith E, Flum David R, Khandelwal Saurabh, Pender John R, Pierson Sheila K, Pories Walter J, Steffen Kristine J, Strain Gladys W, Wolfe Bruce M, Huang Alison J
Department of Obstetrics, Gynecology, and Reproductive Sciences, University of California, San Francisco2Department of Epidemiology and Biostatistics, University of California, San Francisco3Department of Urology, University of California, San Francisco4S.
Department of Epidemiology, University of Pittsburgh Graduate School of Public Health, Pittsburgh, Pennsylvania.
JAMA Intern Med. 2015 Aug;175(8):1378-87. doi: 10.1001/jamainternmed.2015.2609.
Among women and men with severe obesity, evidence for improvement in urinary incontinence beyond the first year after bariatric surgery-induced weight loss is lacking.
To examine change in urinary incontinence before and after bariatric surgery and to identify factors associated with improvement and remission among women and men in the first 3 years after bariatric surgery.
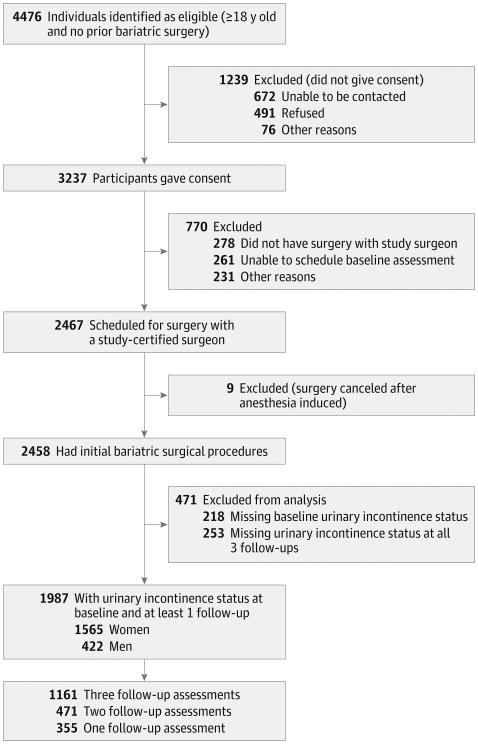
DESIGN, SETTING, AND PARTICIPANTS: The Longitudinal Assessment of Bariatric Surgery 2 is an observational cohort study at 10 US hospitals in 6 geographically diverse clinical centers. Participants were recruited between February 21, 2005, and February 17, 2009. Adults undergoing first-time bariatric surgical procedures as part of clinical care by participating surgeons between March 14, 2006, and April 24, 2009, were followed up for 3 years (through October 24, 2012).
Participants undergoing bariatric surgery completed research assessments before the procedure and annually thereafter.
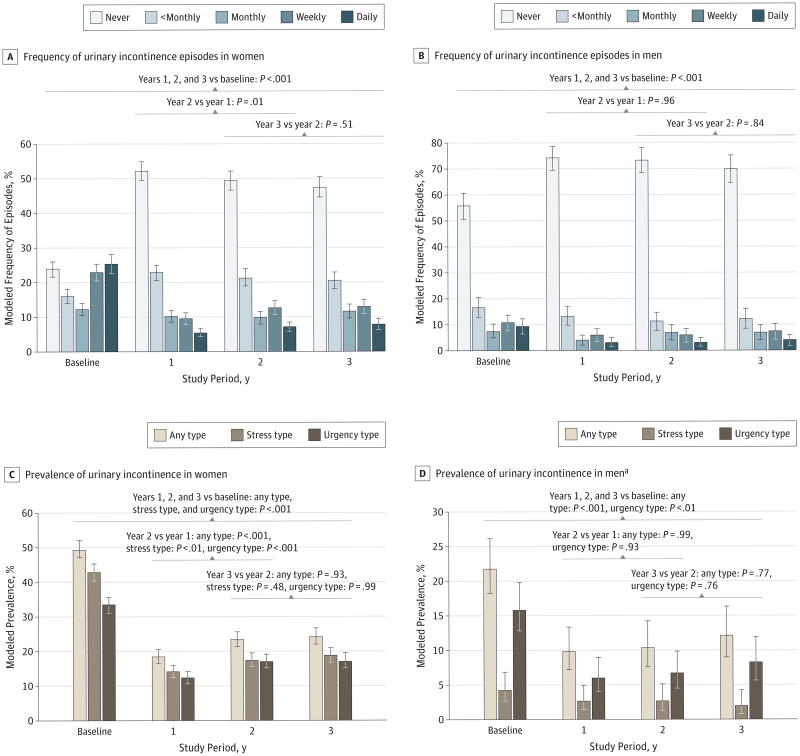
The frequency and type of urinary incontinence episodes in the past 3 months were assessed using a validated questionnaire. Prevalent urinary incontinence was defined as at least weekly urinary incontinence episodes, and remission was defined as change from prevalent urinary incontinence at baseline to less than weekly urinary incontinence episodes at follow-up.
Of 2458 participants, 1987 (80.8%) completed baseline and follow-up assessments. At baseline, the median age was 47 years (age range, 18-78 years), the median body mass index was 46 kg/m2 (range, 34-94 kg/m2), and 1565 of 1987 (78.8%) were women. Urinary incontinence was more prevalent among women (49.3%; 95% CI, 46.9%-51.9%) than men (21.8%; 95% CI, 18.2%-26.1%) (P < .001). After a mean 1-year weight loss of 29.5% (95% CI, 29.0%-30.1%) in women and 27.0% (95% CI, 25.9%-28.6%) in men, year 1 urinary incontinence prevalence was significantly lower among women (18.3%; 95% CI, 16.4%-20.4%) and men (9.8%; 95% CI, 7.2%-13.4%) (P < .001 for all). The 3-year prevalence was higher than the 1-year prevalence for both sexes (24.8%; 95% CI, 21.8%-26.5% among women and 12.2%; 95% CI, 9.0%-16.4% among men) but was substantially lower than baseline (P < .001 for all). Weight loss was independently related to urinary incontinence remission (relative risk, 1.08; 95% CI, 1.06-1.10 in women and 1.07; 95% CI, 1.02-1.13 in men) per 5% weight loss, as were younger age and the absence of a severe walking limitation.
Among women and men with severe obesity, bariatric surgery was associated with substantially reduced urinary incontinence over 3 years. Improvement in urinary incontinence may be an important benefit of bariatric surgery.
在重度肥胖的女性和男性中,缺乏关于减肥手术后一年以上尿失禁改善情况的证据。
研究减肥手术前后尿失禁的变化,并确定减肥手术后3年内女性和男性尿失禁改善和缓解的相关因素。
设计、地点和参与者:减肥手术纵向评估2是一项在6个地理位置不同的临床中心的10家美国医院进行的观察性队列研究。参与者于2005年2月21日至2009年2月17日招募。2006年3月14日至2009年4月24日期间,作为参与外科医生临床护理一部分接受首次减肥手术的成年人接受了3年的随访(至2012年10月24日)。
接受减肥手术的参与者在手术前及此后每年完成研究评估。
使用经过验证的问卷评估过去3个月内尿失禁发作的频率和类型。普遍性尿失禁定义为至少每周发生一次尿失禁发作,缓解定义为从基线时的普遍性尿失禁转变为随访时每周发作少于一次尿失禁。
2458名参与者中,1987名(80.8%)完成了基线和随访评估。基线时,中位年龄为47岁(年龄范围18 - 78岁),中位体重指数为46kg/m²(范围34 - 94kg/m²),1987名参与者中有1565名(78.8%)为女性。女性尿失禁患病率(49.3%;95%CI,46.9% - 51.9%)高于男性(21.8%;95%CI,18.2% - 26.1%)(P <.001)。女性平均减重29.5%(95%CI,29.0% - 30.1%)、男性平均减重27.0%(95%CI,25.9% - 28.6%)后的第1年,女性尿失禁患病率(18.3%;95%CI,16.4% - 20.4%)和男性尿失禁患病率(9.8%;95%CI,7.2% - 13.4%)均显著降低(所有P <.001)。两性的3年患病率均高于1年患病率(女性为24.8%;95%CI,21.8% - 26.5%,男性为12.2%;95%CI,9.0% - 16.4%),但均显著低于基线水平(所有P <.001)。每减重5%,体重减轻与尿失禁缓解独立相关(女性相对风险为1.08;95%CI,1.06 - 1.10,男性为1.07;95%CI,1.02 - 1.13),年龄较小和无严重行走受限情况也与尿失禁缓解相关。
在重度肥胖的女性和男性中,减肥手术与3年内尿失禁显著减少相关。尿失禁的改善可能是减肥手术的一项重要益处。