Saydain Ghulam, Awan Aamir, Manickam Palaniappan, Kleinow Paul, Badr Safwan
Division of Pulmonary and Critical care, Department of Internal Medicine, Detroit Medical Center, Wayne State University, Detroit, MI, USA.
Clin Med Insights Circ Respir Pulm Med. 2015 Jun 23;9:27-33. doi: 10.4137/CCRPM.S22199. eCollection 2015.
Critically ill patients with pulmonary hypertension (PH) pose additional challenges due to the existence of right ventricular (RV) dysfunction. The purpose of this study was to assess the impact of hemodynamic factors on the outcome.
We reviewed the records of patients with a diagnosis of PH admitted to the intensive care unit. In addition to evaluating traditional hemodynamic parameters, we defined severe PH as right atrial pressure >20 mmHg, mean pulmonary artery pressure >55 mmHg, or cardiac index (CI) <2 L/min/m(2). We also defined the RV functional index (RFI) as pulmonary artery systolic pressure (PASP) adjusted for CI as PASP/CI; increasing values reflect RV dysfunction.
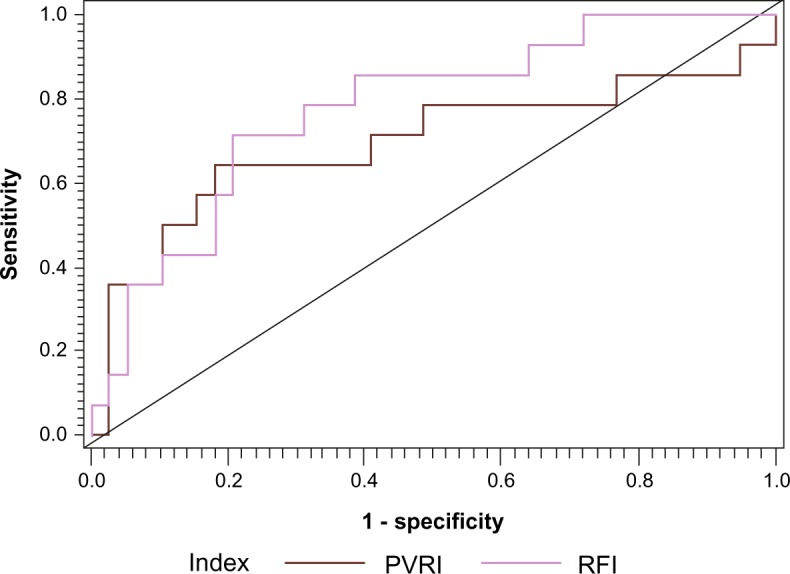
Fifty-three patients (mean age 60 years, 72% women, 79% Blacks), were included in the study. Severe PH was present in 68% of patients who had higher Sequential Organ Failure Assessment (SOFA) score (6.8 ± 3.3 vs 3.8 ± 1.6; P = 0.001) and overall in-hospital mortality (36% vs 6%; P = 0.02) compared to nonsevere patients, although Acute Physiology and Chronic Health Evaluation (APACHE) II scores (19.9 ± 7.5 vs 18.5 ± 6.04; P = 0.52) were similar and sepsis was more frequent among nonsevere PH patients (31 vs 64%; P = 0.02). Severe PH (P = 0.04), lower mean arterial pressure (P = 0.04), and CI (P = 0.01); need for invasive ventilation (P = 0.02) and vasopressors (P = 0.03); and higher SOFA (P = 0.001), APACHE II (P = 0.03), pulmonary vascular resistance index (PVRI) (P = 0.01), and RFI (P = 0.004) were associated with increased mortality. In a multivariate model, SOFA [OR = 1.45, 95% confidence interval (C.I.) = 1.09-1.93; P = 0.01], PVRI (OR = 1.12, 95% C.I. = 1.02-1.24; P = 0.02), and increasing RFI (OR = 1.06, 95% C.I. = 1.01-1.11; P = 0.01) were independently associated with mortality.
PH is an independent risk factor for mortality in critically ill patients. Composite factors rather than individual hemodynamic parameters are better predictors of outcome. Monitoring of RV function using composite hemodynamic factors resulting in specific interventions is likely to improve survival and needs to be studied further.
由于存在右心室(RV)功能障碍,患有肺动脉高压(PH)的重症患者面临更多挑战。本研究的目的是评估血流动力学因素对预后的影响。
我们回顾了入住重症监护病房且诊断为PH的患者记录。除了评估传统血流动力学参数外,我们将严重PH定义为右心房压力>20 mmHg、平均肺动脉压力>55 mmHg或心脏指数(CI)<2 L/min/m²。我们还将右心室功能指数(RFI)定义为经CI校正的肺动脉收缩压(PASP),即PASP/CI;数值增加反映右心室功能障碍。
53例患者(平均年龄60岁,72%为女性,79%为黑人)纳入研究。与非严重PH患者相比,68%的严重PH患者序贯器官衰竭评估(SOFA)评分更高(6.8±3.3对3.8±1.6;P = 0.001),总体住院死亡率更高(36%对6%;P = 0.02),尽管急性生理与慢性健康状况评估(APACHE)II评分相似(19.9±7.5对18.5±6.04;P = 0.52),且非严重PH患者中脓毒症更常见(31%对64%;P = 0.02)。严重PH(P = 0.04)、较低的平均动脉压(P = 0.04)和CI(P = 0.01);需要有创通气(P = 0.02)和血管加压药(P = 0.03);以及较高的SOFA(P = 0.001)、APACHE II(P = 0.03)、肺血管阻力指数(PVRI)(P = 0.01)和RFI(P = 0.004)与死亡率增加相关。在多变量模型中,SOFA [比值比(OR)= 1.45,95%置信区间(C.I.)= 1.09 - 1.93;P = 0.01]、PVRI(OR = 1.12,95% C.I. = 1.02 - 1.24;P = 0.02)以及RFI升高(OR = 1.06,95% C.I. = 1.01 - 1.11;P = 0.01)与死亡率独立相关。
PH是重症患者死亡的独立危险因素。综合因素而非单个血流动力学参数是更好的预后预测指标。使用综合血流动力学因素监测右心室功能并进行特定干预可能会提高生存率,这需要进一步研究。