Puiggròs Carolina, Molinos Rosa, Ortiz M Dolors, Ribas Montserrat, Romero Carlos, Vázquez Concepcion, Segurola Hegoi, Burgos Rosa
Nutritional Support Unit, Vall d'Hebron University Hospital, Barcelona, Spain
Nutritional Support Unit, Vall d'Hebron University Hospital, Barcelona, Spain.
Nutr Clin Pract. 2015 Dec;30(6):815-23. doi: 10.1177/0884533615592954. Epub 2015 Jul 24.
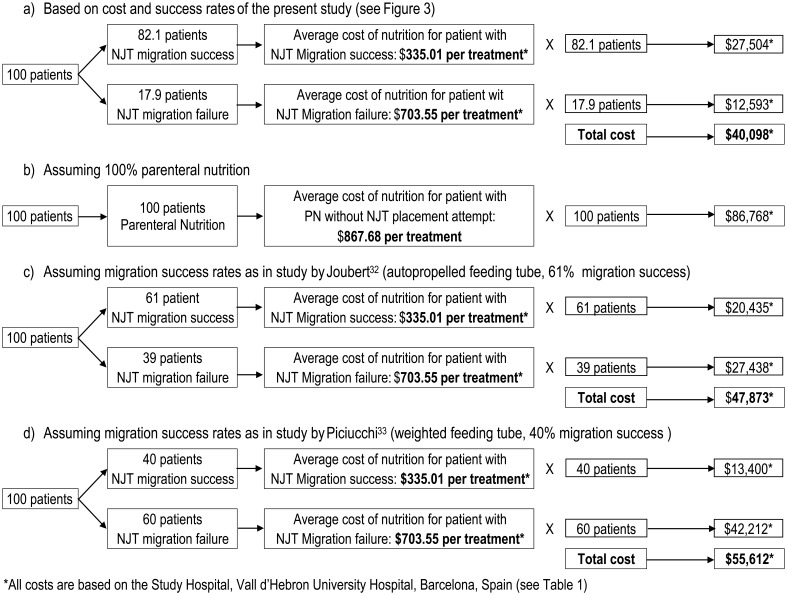
The procedures needed to insert nasojejunal tubes (NJTs) are often invasive or uncomfortable for the patient and require hospital resources. The objectives of this study were to describe our experience in inserting a self-propelling NJT with distal pigtail end and evaluate clinical validity and cost efficacy of this enteral nutrition (EN) approach compared with parenteral nutrition (PN).
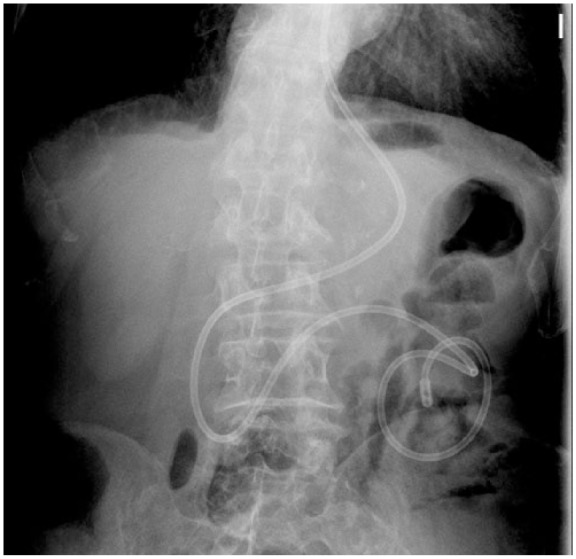
Prospective study from July 2009 to December 2010, including hospitalized noncritical patients who required short-term jejunal EN. The tubes were inserted at bedside, using intravenous erythromycin as a prokinetic drug. Positioning was considered correct when the distal end was beyond the ligament of Treitz. Migration failure was considered when the tube was not positioned into the jejunum within 48 hours postinsertion.
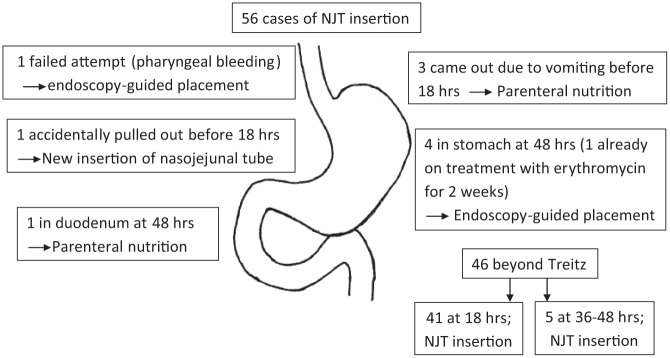
Fifty-six insertions were recorded in 47 patients, most frequently in severe acute pancreatitis (69.6%). The migration rates at 18 and 48 hours postinsertion were 73.2% and 82.1%, respectively. There was migration failure in 8.9% of cases, and 8.9% were classified null (the tube was no longer in the gastrointestinal tract at 18 hours). There were no reported or observed complications. The mean duration of the EN was 12 ± 10.8 days. Five different types of EN formula were used. The total study cost was 53.9% lower compared with using PN in all patients.
Our study demonstrated that bedside insertion of a self-propelling NJT is a safe, cost-effective, and successful technique for postpyloric enteral feeding in at least 73% of the patients, and only 18% of patients could eventually need other placement techniques. It can avoid the need for more aggressive or expensive placement techniques or even PN if we cannot achieve enteral access.
插入鼻空肠管(NJTs)所需的操作通常对患者具有侵入性或会让患者感到不适,并且需要医院资源。本研究的目的是描述我们插入带有远端猪尾的自行推进式鼻空肠管的经验,并评估这种肠内营养(EN)方法与肠外营养(PN)相比的临床有效性和成本效益。
2009年7月至2010年12月的前瞻性研究,纳入需要短期空肠肠内营养的住院非危重症患者。在床边插入鼻空肠管,使用静脉注射红霉素作为促动力药物。当远端超过Treitz韧带时,定位被认为正确。插入后48小时内鼻空肠管未进入空肠时,视为置管失败。
47例患者共进行了56次置管,最常见于重症急性胰腺炎患者(69.6%)。插入后18小时和48小时的置管成功率分别为73.2%和82.1%。8.9%的病例出现置管失败,8.9%被分类为无效(18小时时鼻空肠管不再位于胃肠道内)。未报告或观察到并发症。肠内营养的平均持续时间为12±10.8天。使用了五种不同类型的肠内营养配方。与所有患者使用肠外营养相比,总研究成本降低了53.9%。
我们的研究表明,床边插入自行推进式鼻空肠管是一种安全、经济有效的技术,至少73%的患者行幽门后置管喂养成功,只有18%的患者最终可能需要其他置管技术。如果我们无法实现肠内通路,这种方法可以避免使用更激进或昂贵的置管技术甚至肠外营养。