Parikh Shital N, Lykissas Marios G, Roshdy Mazen, Mineo Ronald C, Wall Eric J
Division of Orthopaedic Surgery, Cincinnati Children's Hospital Medical Center, 3333 Burnet Avenue MLC 2017, Cincinnati, OH, 45229, USA,
J Child Orthop. 2015 Aug;9(4):295-302. doi: 10.1007/s11832-015-0674-8. Epub 2015 Aug 9.
The purpose of our study was to determine the long-term functional outcomes of pin tract infection after percutaneous pinning of displaced supracondylar humeral fractures in children, and to evaluate the potential for intracapsular pin placement based on pin configuration in cadaveric elbows.
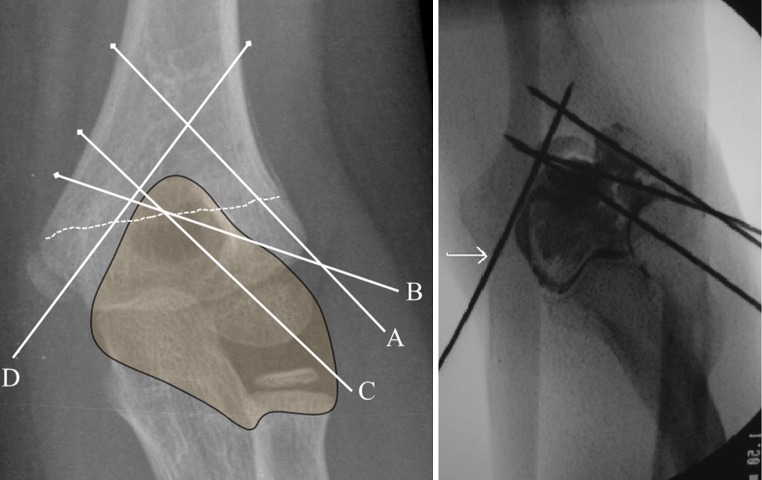
We conducted a retrospective review of all patients requiring percutaneous pinning in a single institution over a 19-year period. The functional outcome assessment consisted of a telephone interview using the Disabilities of the Arm, Shoulder and Hand (DASH)] Outcome Measure and the Patient-Rated Elbow Evaluation (PREE) questionnaires. The risk of intracapsular pin placement was studied in cadaveric elbows for the three most common pin configurations: divergent lateral, parallel lateral, and medial and lateral crossed pins.
Of 490 children, 21 (4.3 %) developed pin tract infection. There were 15 (3.1 %) superficial and six (1.2 %) deep infections (osteomyelitis and septic arthritis). Both DASH and PREE scores were excellent at a mean of 18 years post-surgery. The risk of intracapsular pin placement using parallel lateral pins was found to be greater (p < 0.05) than either crossed or divergent lateral pinning configurations.
Most infections after pinning of supracondylar humerus fractures are superficial and can be managed with pin removal, oral antibiotics, and local wound care. Septic arthritis and osteomyelitis are rare complications; when they do occur, they seem to be associated with parallel lateral pin configuration, though a causal relationship could not be established from the current study. Satisfactory long-term outcomes of these deep infections can be expected when treated aggressively with surgical debridement and intravenous antibiotics.
我们研究的目的是确定儿童肱骨髁上骨折经皮穿针固定术后针道感染的长期功能结局,并根据尸体肘部的针配置评估关节内穿针的可能性。
我们对一家机构19年间所有需要经皮穿针固定的患者进行了回顾性研究。功能结局评估包括使用手臂、肩部和手部功能障碍(DASH)结局测量法和患者自评肘部评估(PREE)问卷进行电话访谈。在尸体肘部研究了三种最常见的针配置导致关节内穿针的风险:外侧发散、外侧平行以及内侧和外侧交叉针。
490名儿童中,21名(4.3%)发生了针道感染。有15名(3.1%)为浅表感染,6名(1.2%)为深部感染(骨髓炎和化脓性关节炎)。术后平均18年时,DASH和PREE评分均极佳。发现使用外侧平行针进行关节内穿针的风险高于交叉或外侧发散针配置(p<0.05)。
肱骨髁上骨折穿针固定术后的大多数感染为浅表感染,可通过拔针、口服抗生素和局部伤口护理进行处理。化脓性关节炎和骨髓炎是罕见的并发症;当它们确实发生时,似乎与外侧平行针配置有关,尽管从当前研究中无法确定因果关系。积极进行手术清创和静脉使用抗生素治疗时,有望获得这些深部感染令人满意的长期结局。