Zhang Zhen-Yu, Chan Aden Ka-Yin, Ding Xiao-Jie, Qin Zhi-Yong, Hong Christopher S, Chen Ling-Chao, Zhang Xin, Zhao Fang-Ping, Wang Yin, Wang Yang, Zhou Liang-Fu, Zhuang Zhengping, Ng Ho-Keung, Yan Hai, Yao Yu, Mao Ying
Department of Neurosurgery, Huashan Hospital, Fudan University, Shanghai, China.
Department of Anatomical and Cellular Pathology, Prince of Wales Hospital, The Chinese University of Hong Kong, Shatin, N.T., Hong Kong, China.
Oncotarget. 2015 Sep 22;6(28):24871-83. doi: 10.18632/oncotarget.4549.
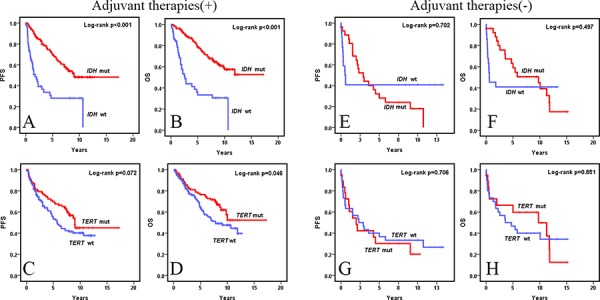
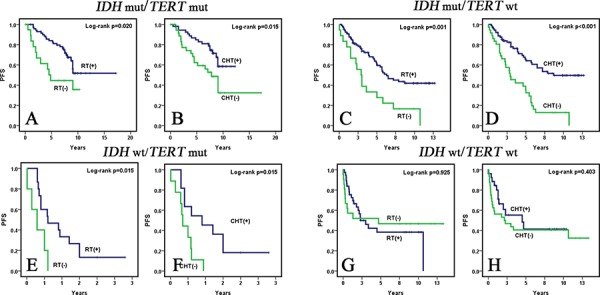
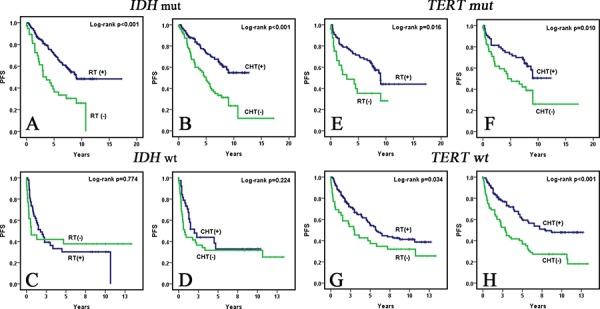
IDH mutations frequently occur in WHO grade II and III diffuse gliomas and have favorable prognosis compared to wild-type tumors. However, whether IDH mutations in WHO grade II and II diffuse gliomas predict enhanced sensitivity to adjuvant radiation (RT) or chemotherapy (CHT) is still being debated. Recent studies have identified recurrent mutations in the promoter region of telomerase reverse transcriptase (TERT) in gliomas. We previously demonstrated that TERT promoter mutations may be promising biomarkers in glioma survival prognostication when combined with IDH mutations. This study analyzed IDH and TERT promoter mutations in 295 WHO grade II and III diffuse gliomas treated with or without adjuvant therapies to explore their impact on the sensitivity of tumors to genotoxic therapies. IDH mutations were found in 216 (73.2%) patients and TERT promoter mutations were found in 112 (38%) patients. In multivariate analysis, IDH mutations (p < 0.001) were independent prognostic factors for PFS and OS in patients receiving genotoxic therapies while TERT promoter mutations were not. In univariate analysis, IDH and TERT promoter mutations were not significant prognostic factors in patients who did not receive genotoxic therapies. Adjuvant RT and CHT were factors independently impacting PFS (RT p = 0.001, CHT p = 0.026) in IDH mutated WHO grade II and III diffuse gliomas but not in IDH wild-type group. Univariate and multivariate analyses demonstrated TERT promoter mutations further stratified IDH wild-type WHO grade II and III diffuse gliomas into two subgroups with different responses to genotoxic therapies. Adjuvant RT and CHT were significant parameters influencing PFS in the IDH wt/TERT mut subgroup (RT p = 0.015, CHT p = 0.015) but not in the IDH wt/TERT wt subgroup. Our data demonstrated that IDH mutated WHO grade II and III diffuse gliomas had better PFS and OS than their IDH wild-type counterparts when genotoxic therapies were administered after surgery. Importantly, we also found that TERT promoter mutations further stratify IDH wild-type WHO grade II and III diffuse gliomas into two subgroups with different responses to adjuvant therapies. Taken together, TERT promoter mutations may predict enhanced sensitivity to genotoxic therapies in IDH wild-type WHO grade II and III diffuse gliomas and may justify intensified treatment in this subgroup.
异柠檬酸脱氢酶(IDH)突变频繁发生于世界卫生组织(WHO)二级和三级弥漫性胶质瘤中,与野生型肿瘤相比,其预后较好。然而,WHO二级和三级弥漫性胶质瘤中的IDH突变是否预示着对辅助放疗(RT)或化疗(CHT)的敏感性增强仍存在争议。最近的研究已经确定了胶质瘤中端粒酶逆转录酶(TERT)启动子区域的复发性突变。我们之前证明,TERT启动子突变与IDH突变联合时,可能是胶质瘤生存预后中有前景的生物标志物。本研究分析了295例接受或未接受辅助治疗的WHO二级和三级弥漫性胶质瘤中的IDH和TERT启动子突变,以探讨它们对肿瘤对基因毒性治疗敏感性的影响。在216例(73.2%)患者中发现了IDH突变,在112例(38%)患者中发现了TERT启动子突变。在多变量分析中,IDH突变(p < 0.001)是接受基因毒性治疗患者无进展生存期(PFS)和总生存期(OS)的独立预后因素,而TERT启动子突变则不是。在单变量分析中,IDH和TERT启动子突变在未接受基因毒性治疗的患者中不是显著的预后因素。辅助RT和CHT是影响IDH突变的WHO二级和三级弥漫性胶质瘤PFS的独立因素(RT p = 0.001,CHT p = 0.026),但在IDH野生型组中不是。单变量和多变量分析表明,TERT启动子突变进一步将IDH野生型的WHO二级和三级弥漫性胶质瘤分为两个对基因毒性治疗反应不同的亚组。辅助RT和CHT是影响IDH野生型/TERT突变亚组PFS的显著参数(RT p = 0.015,CHT p = 0.015),但在IDH野生型/TERT野生型亚组中不是。我们的数据表明,术后给予基因毒性治疗时,IDH突变的WHO二级和三级弥漫性胶质瘤的PFS和OS比其IDH野生型对应物更好。重要的是,我们还发现TERT启动子突变进一步将IDH野生型的WHO二级和三级弥漫性胶质瘤分为两个对辅助治疗反应不同的亚组。综上所述,TERT启动子突变可能预示着IDH野生型的WHO二级和三级弥漫性胶质瘤对基因毒性治疗的敏感性增强,并可能证明该亚组强化治疗的合理性。