Mandelli Sara, Riva Emma, Tettamanti Mauro, Detoma Paolo, Giacomin Adriano, Lucca Ugo
Laboratory of Geriatric Neuropsychiatry, IRCCS-Istituto di Ricerche Farmacologiche "Mario Negri", Milan, Italy.
Laboratory of Analysis, Ospedale degli Infermi, Biella, Italy.
PLoS One. 2015 Aug 28;10(8):e0136039. doi: 10.1371/journal.pone.0136039. eCollection 2015.
Kidney function declines considerably with age, but little is known about its clinical significance in the oldest-old.
To study the association between reduced glomerular filtration rate (GFR) estimated according to five equations with mortality in the oldest-old.
Prospective population-based study.
Municipality of Biella, Piedmont, Italy.
700 subjects aged 85 and older participating in the "Health and Anemia" Study in 2007-2008.
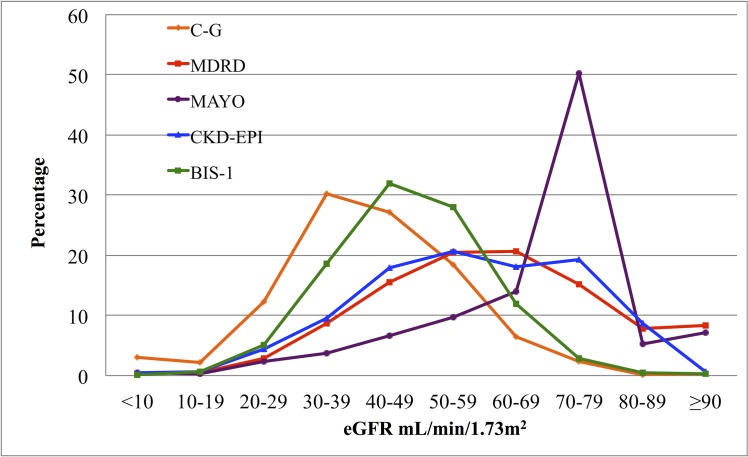
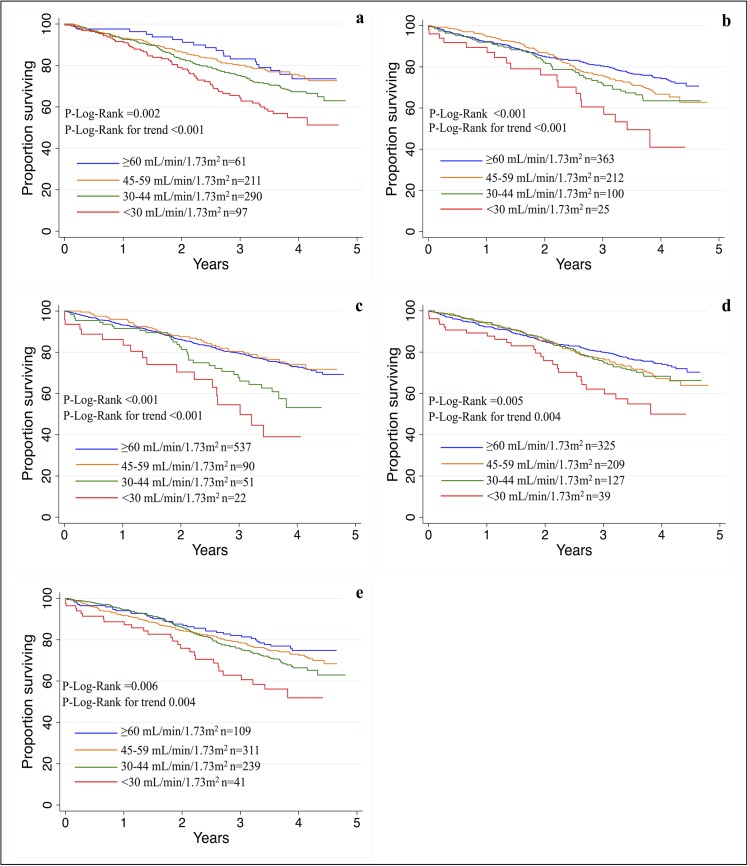
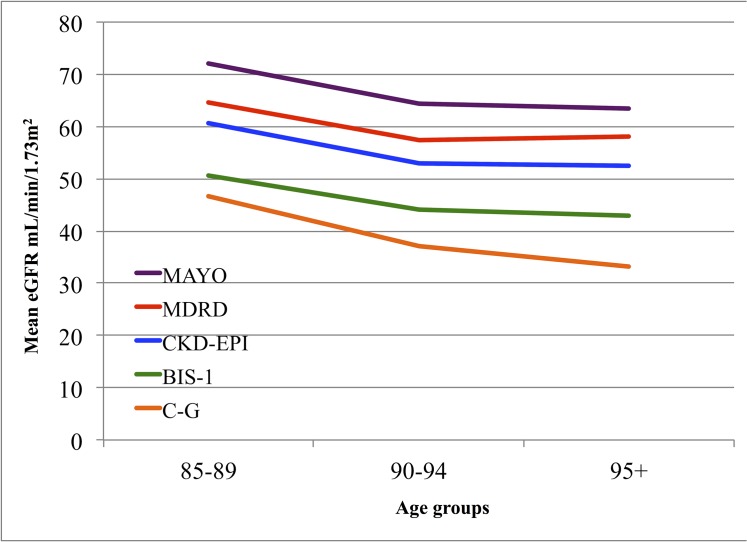
GFR was estimated using five creatinine-based equations: the Cockcroft-Gault (C-G), Modification of Diet in Renal Disease (MDRD), MAYO Clinic, Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) and Berlin Initiative Study-1 (BIS-1). Survival analysis was used to study mortality in subjects with reduced eGFR (<60 mL/min/1.73 m(2)) compared to subjects with eGFR ≥ 60 mL/min/1.73 m(2).
Prevalence of reduced GFR was 90.7% with the C-G, 48.1% with MDRD, 23.3% with MAYO, 53.6% with CKD-EPI and 84.4% with BIS-1. After adjustment for confounders, two-year mortality was significantly increased in subjects with reduced eGFR using BIS-1 and C-G equations (adjusted HRs: 2.88 and 3.30, respectively). Five-year mortality was significantly increased in subjects with eGFR <60 mL/min/1.73 m(2) using MAYO, CKD-EPI and, in a graduated fashion in reduced eGFR categories, MDRD. After 5 years, oldest old with an eGFR <30 mL/min/1.73 m(2) showed a significantly higher risk of death whichever equation was used (adjusted HRs between 2.04 and 2.70).
In the oldest old, prevalence of reduced eGFR varies noticeably depending on the equation used. In this population, risk of mortality was significantly higher for reduced GFR estimated with the BIS-1 and C-G equations over the short term. Though after five years the MDRD appeared on the whole a more consistent predictor, differences in mortality prediction among equations over the long term were less apparent. Noteworthy, subjects with a severely reduced GFR were consistently at higher risk of death regardless of the equation used to estimate GFR.
肾功能会随着年龄的增长而显著下降,但对于其在高龄老人中的临床意义却知之甚少。
研究根据五种公式估算的肾小球滤过率(GFR)降低与高龄老人死亡率之间的关联。
基于人群的前瞻性研究。
意大利皮埃蒙特比耶拉市。
700名年龄在85岁及以上的受试者,于2007 - 2008年参与“健康与贫血”研究。
使用基于肌酐的五种公式估算GFR:Cockcroft - Gault(C - G)公式、肾脏病饮食改良(MDRD)公式、梅奥诊所公式、慢性肾脏病流行病学协作组(CKD - EPI)公式和柏林倡议研究 - 1(BIS - 1)公式。生存分析用于研究估算肾小球滤过率(eGFR)降低(<60 mL/min/1.73 m²)的受试者与eGFR≥60 mL/min/1.73 m²的受试者的死亡率。
使用C - G公式估算的GFR降低的患病率为90.7%,MDRD公式为48.1%,梅奥诊所公式为23.3%,CKD - EPI公式为53.6%,BIS - 1公式为84.4%。在对混杂因素进行调整后,使用BIS - 1和C - G公式估算eGFR降低的受试者的两年死亡率显著增加(调整后的风险比分别为2.88和3.30)。使用梅奥诊所公式、CKD - EPI公式以及在eGFR降低类别中呈梯度变化的MDRD公式估算,eGFR <60 mL/min/1.73 m²的受试者的五年死亡率显著增加。五年后,无论使用哪种公式,eGFR <30 mL/min/(1.73 m²)的高龄老人的死亡风险均显著更高(调整后的风险比在2.04至2.70之间)。
在高龄老人中,根据所使用的公式不同,估算肾小球滤过率降低的患病率有显著差异。在这一人群中,短期内使用BIS - 1和C - G公式估算的GFR降低的死亡风险显著更高。尽管五年后MDRD公式总体上似乎是一个更一致的预测指标,但长期来看各公式在死亡率预测方面的差异不太明显。值得注意的是,无论使用哪种公式估算GFR,GFR严重降低的受试者始终具有更高的死亡风险。