Gubhaju Lina, Banks Emily, MacNiven Rona, McNamara Bridgette J, Joshy Grace, Bauman Adrian, Eades Sandra J
Aboriginal Health, Baker IDI Heart and Diabetes Institute, 99 Commercial Road, Melbourne, 3004, Victoria, Australia.
Chronic Disease Epidemiology, National Centre for Epidemiology and Population Health, The Australian National University, Acton, 2601, Australian Capital Territory, Australia.
PLoS One. 2015 Sep 30;10(9):e0139364. doi: 10.1371/journal.pone.0139364. eCollection 2015.
Australian Aboriginal people are disproportionately affected by physical disability; the reasons for this are unclear. This study aimed to quantify associations between severe physical functional limitations and socio-demographic and health-related factors among older Aboriginal and non-Aboriginal adults.
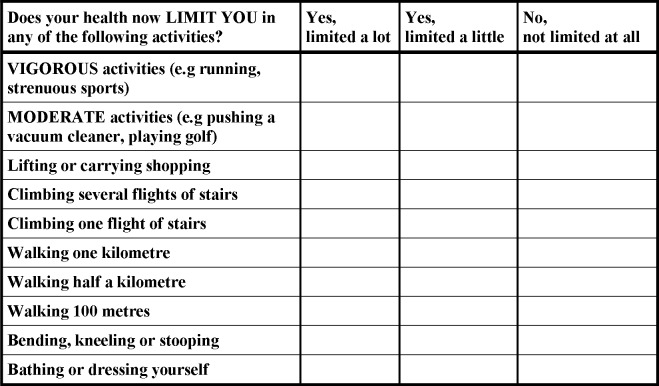
Questionnaire data from 1,563 Aboriginal and 226,802 non-Aboriginal participants aged ≥45 years from the Sax Institute's 45 and Up Study (New South Wales, Australia) were used to calculate age- and sex-adjusted prevalence ratios (aPRs) for severe limitation [MOS-PF score <60] according to socio-demographic and health-related factors.
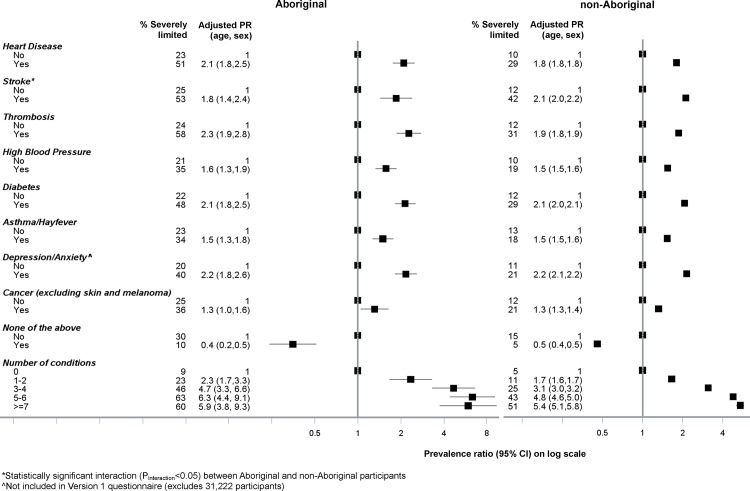
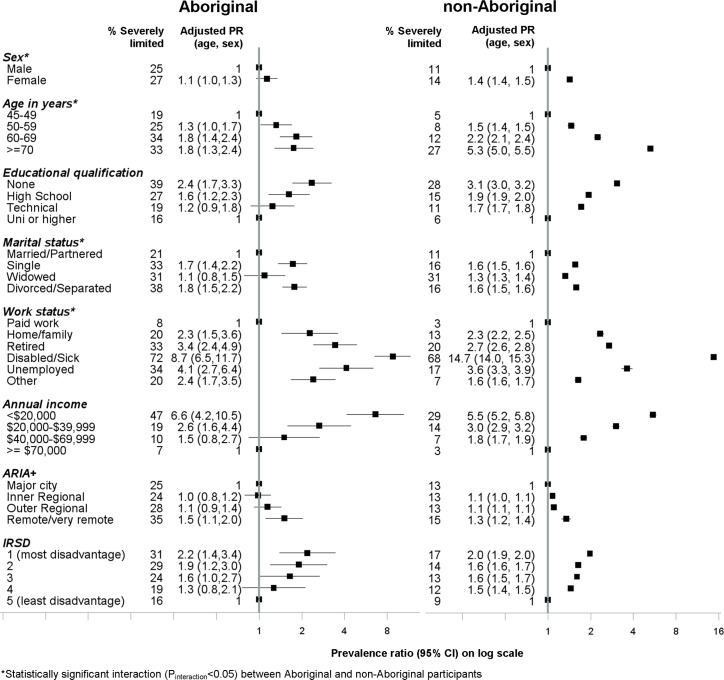
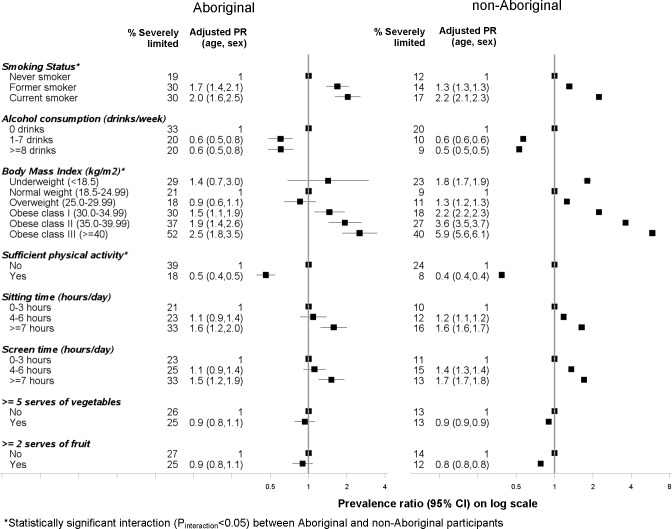
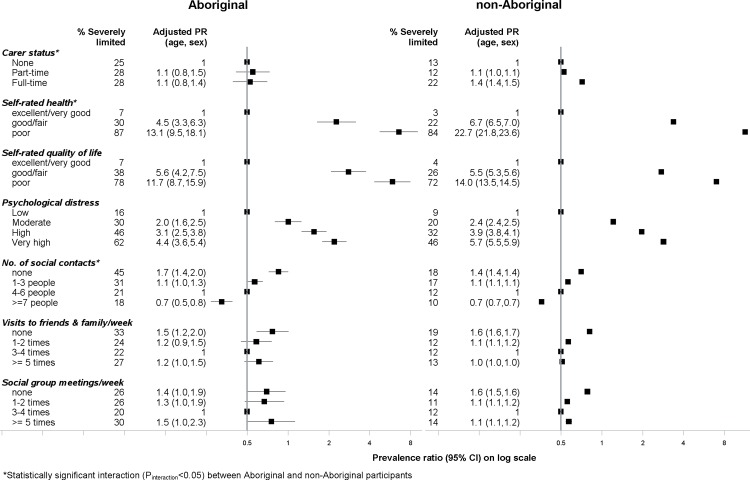
Overall, 26% (410/1563) of Aboriginal participants and 13% (29,569/226,802) of non-Aboriginal participants had severe limitations (aPR 2.8, 95%CI 2.5-3.0). In both Aboriginal and non-Aboriginal participants, severe limitation was significantly associated with: being ≥70 vs <70 years old (aPRs 1.8, 1.3-2.4 and 5.3, 5.0-5.5, within Aboriginal and non-Aboriginal participants, respectively), none vs tertiary educational qualifications (aPRs 2.4, 1.7-3.3 and 3.1, 3.0-3.2), lower vs higher income (aPRs 6.6, 4.2-10.5 and 5.5, 5.2-5.8), current vs never-smoking (aPRs 2.0, 1.6-2.5 and 2.2, 2.1-2.3), obese vs normal weight (aPRs 1.7, 1.3-2.2 and 2.7, 2.7-2.8) and sitting for ≥7 vs <7 hours/day (aPRs 1.6, 1.2-2.0 and 1.6, 1.6-1.7). Severe limitations increased with increasing ill-health, with aPRs rising to 5-6 for ≥5 versus no chronic conditions. It was significantly higher in those with few vs many social contacts (aPRs 1.7, 1.4-2.0 and 1.4, 1.4-1.4) and with very high vs low psychological distress (aPRs 4.4, 3.6-5.4 and 5.7, 5.5-5.9).
Although the prevalence of severe physical limitation among Aboriginal people in this study is around three-fold that of non-Aboriginal people, the factors related to it are similar, indicating that Aboriginal people have higher levels of risk factors for and consequences of severe limitations. Effective management of chronic disease and reducing the prevalence of obesity and smoking are important areas for attention.
澳大利亚原住民受身体残疾影响的比例过高,其原因尚不清楚。本研究旨在量化老年原住民和非原住民成年人中严重身体功能受限与社会人口学及健康相关因素之间的关联。
来自萨克斯研究所45岁及以上研究(澳大利亚新南威尔士州)的1563名原住民和226802名非原住民参与者的问卷数据,用于根据社会人口学和健康相关因素计算严重受限[MOS-PF评分<60]的年龄和性别调整患病率比(aPRs)。
总体而言,26%(410/1563)的原住民参与者和13%(29569/226802)的非原住民参与者有严重受限(aPR 2.8,95%CI 2.5-3.0)。在原住民和非原住民参与者中,严重受限均与以下因素显著相关:年龄≥70岁与<70岁(原住民和非原住民参与者中aPRs分别为1.8,1.3-2.4和5.3,5.0-5.5)、无高等教育学历与有高等教育学历(aPRs分别为2.4,1.7-3.3和3.1,3.0-3.2)、低收入与高收入(aPRs分别为6.6,4.2-10.5和5.5,5.2-5.8)、当前吸烟者与从不吸烟者(aPRs分别为2.0,1.6-2.5和2.2,2.1-2.3)、肥胖与正常体重(aPRs分别为1.7,1.3-2.2和2.7,2.7-2.8)以及每天久坐≥7小时与<7小时(aPRs分别为1.6,1.2-2.0和1.6,1.6-1.7)。严重受限随健康状况变差而增加,慢性病≥5种与无慢性病相比aPRs升至5-6。社交接触少与社交接触多的人群中严重受限显著更高(aPRs分别为1.7,1.4-2.0和1.4,1.4-1.4),心理困扰非常高与低的人群中严重受限也显著更高(aPRs分别为4.4,3.6-5.4和5.7,5.5-5.9)。
尽管本研究中原住民严重身体受限的患病率约为非原住民的三倍,但其相关因素相似,表明原住民严重受限的风险因素水平及后果更高。有效管理慢性病以及降低肥胖和吸烟患病率是重要的关注领域。