Tan Timothy C, Flynn Aidan W, Chen-Tournoux Annabel, Rudski Lawrence G, Mehrotra Praveen, Nunes Maria C, Rincon Luis M, Shahian David M, Picard Michael H, Afilalo Jonathan
Massachusetts General Hospital, Harvard Medical School, Boston, MA (T.C.T., A.W.F., P.M., M.C.N., L.M.R., D.M.S., M.H.P., J.A.).
Massachusetts General Hospital, Harvard Medical School, Boston, MA (T.C.T., A.W.F., P.M., M.C.N., L.M.R., D.M.S., M.H.P., J.A.) Hartford Hospital, University of Connecticut, Hartford, CT (A.W.F.).
J Am Heart Assoc. 2015 Oct 26;4(10):e002129. doi: 10.1161/JAHA.115.002129.
Risk prediction is a critical step in patient selection for aortic valve replacement (AVR), yet existing risk scores incorporate very few echocardiographic parameters. We sought to evaluate the incremental predictive value of a complete echocardiogram to identify high-risk surgical candidates before AVR.
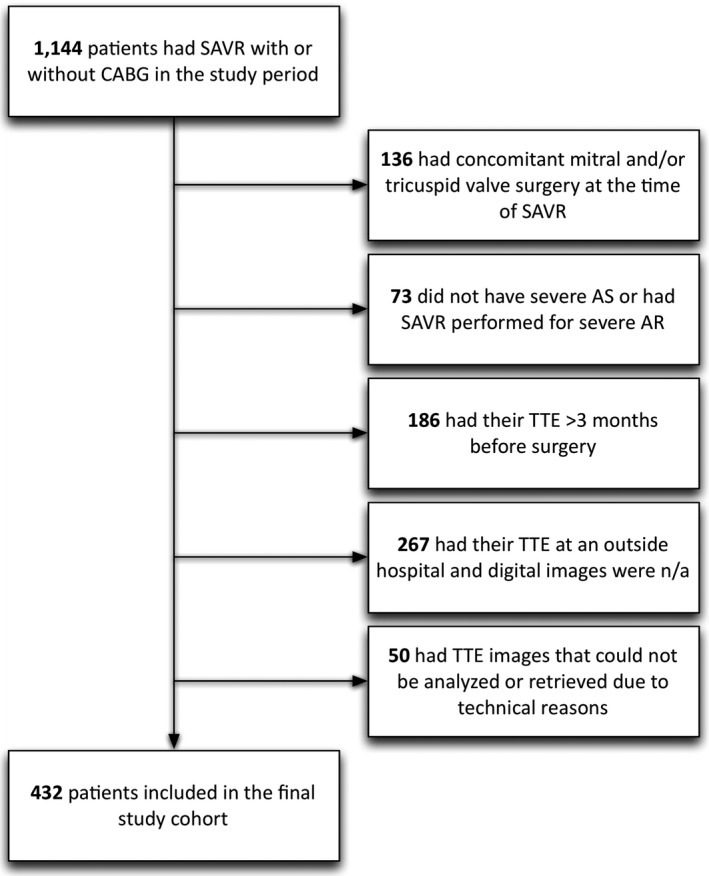
A cohort of patients with severe aortic stenosis undergoing surgical AVR with or without coronary bypass was assembled at 2 tertiary centers. Preoperative echocardiograms were reviewed by independent observers to quantify chamber size/function and valve function. Patient databases were queried to extract clinical data. The cohort consisted of 432 patients with a mean age of 73.5 years and 38.7% females. Multivariable logistic regression revealed 3 echocardiographic predictors of in-hospital mortality or major morbidity: E/e' ratio reflective of elevated left ventricular (LV) filling pressure; myocardial performance index reflective of right ventricular (RV) dysfunction; and small LV end-diastolic cavity size. Addition of these echocardiographic parameters to the STS risk score led to an integrated discrimination improvement of 4.1% (P<0.0001). After a median follow-up of 2 years, Cox regression revealed 5 echocardiographic predictors of all-cause mortality: small LV end-diastolic cavity size; LV mass index; mitral regurgitation grade; right atrial area index; and mean aortic gradient <40 mm Hg.
Echocardiographic measures of LV diastolic dysfunction and RV performance add incremental value to the STS risk score and should be integrated in prediction when evaluating the risk of AVR. In addition, findings of small hypertrophied LV cavities and/or low mean aortic gradients confer a higher risk of 2-year mortality.
风险预测是主动脉瓣置换术(AVR)患者选择过程中的关键步骤,但现有的风险评分纳入的超声心动图参数极少。我们试图评估完整超声心动图在识别AVR术前高危手术候选者方面的增量预测价值。
在2个三级中心组建了一组接受有或无冠状动脉搭桥手术AVR的重度主动脉瓣狭窄患者队列。独立观察者对术前超声心动图进行评估,以量化心腔大小/功能和瓣膜功能。查询患者数据库以提取临床数据。该队列由432例患者组成,平均年龄73.5岁,女性占38.7%。多变量逻辑回归显示3个院内死亡或主要并发症的超声心动图预测因素:反映左心室(LV)充盈压升高的E/e'比值;反映右心室(RV)功能障碍的心肌性能指数;以及小的LV舒张末期腔径。将这些超声心动图参数添加到STS风险评分中,综合辨别力提高了4.1%(P<0.0001)。中位随访2年后,Cox回归显示5个全因死亡的超声心动图预测因素:小的LV舒张末期腔径;LV质量指数;二尖瓣反流分级;右心房面积指数;以及平均主动脉梯度<40 mmHg。
LV舒张功能障碍和RV性能的超声心动图测量为STS风险评分增加了增量价值,在评估AVR风险时应纳入预测。此外,小的肥厚LV腔和/或低平均主动脉梯度的发现提示2年死亡率风险更高。