Awad Susanne F, Sgaier Sema K, Ncube Gertrude, Xaba Sinokuthemba, Mugurungi Owen M, Mhangara Mutsa M, Lau Fiona K, Mohamoud Yousra A, Abu-Raddad Laith J
Infectious Disease Epidemiology Group, Weill Cornell Medical College in Qatar, Cornell University, Qatar Foundation, Education City, Doha, Qatar.
Integrated Delivery, Global Development Program, Bill & Melinda Gates Foundation, Seattle, Washington, United States of America; Department of Global Health, University of Washington, Seattle, Washington, United States of America.
PLoS One. 2015 Nov 3;10(11):e0140818. doi: 10.1371/journal.pone.0140818. eCollection 2015.
The voluntary medical male circumcision (VMMC) program in Zimbabwe aims to circumcise 80% of males aged 13-29 by 2017. We assessed the impact of actual VMMC scale-up to date and evaluated the impact of potential alterations to the program to enhance program efficiency, through prioritization of subpopulations.
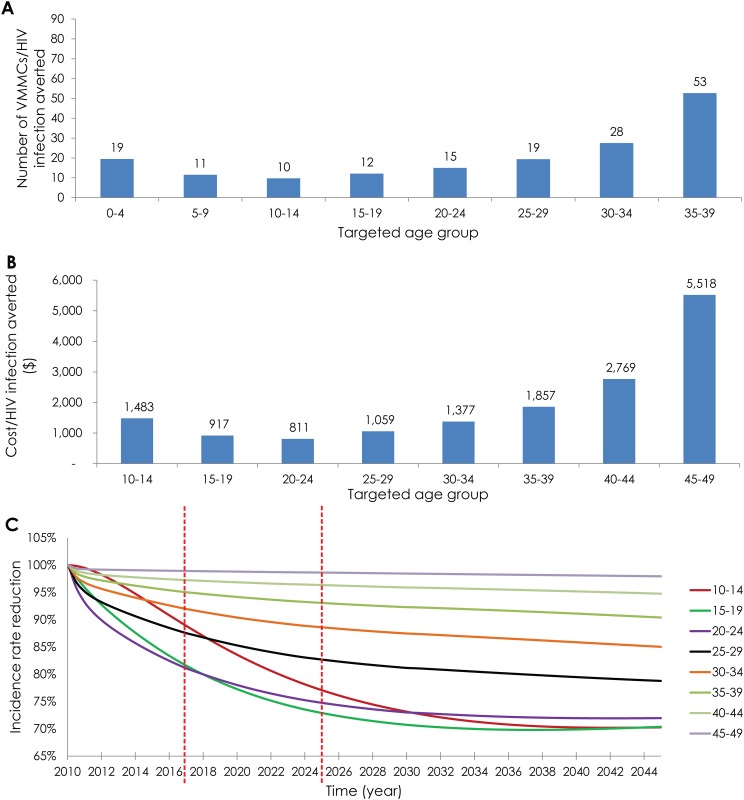
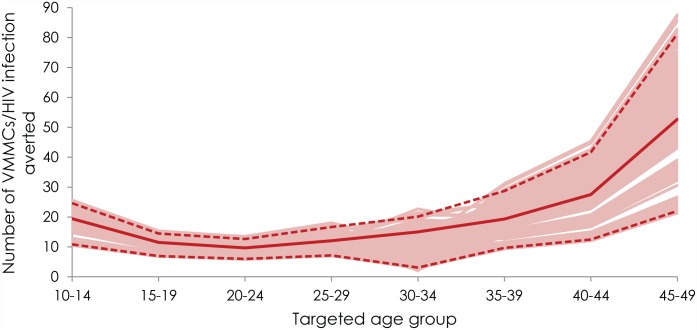
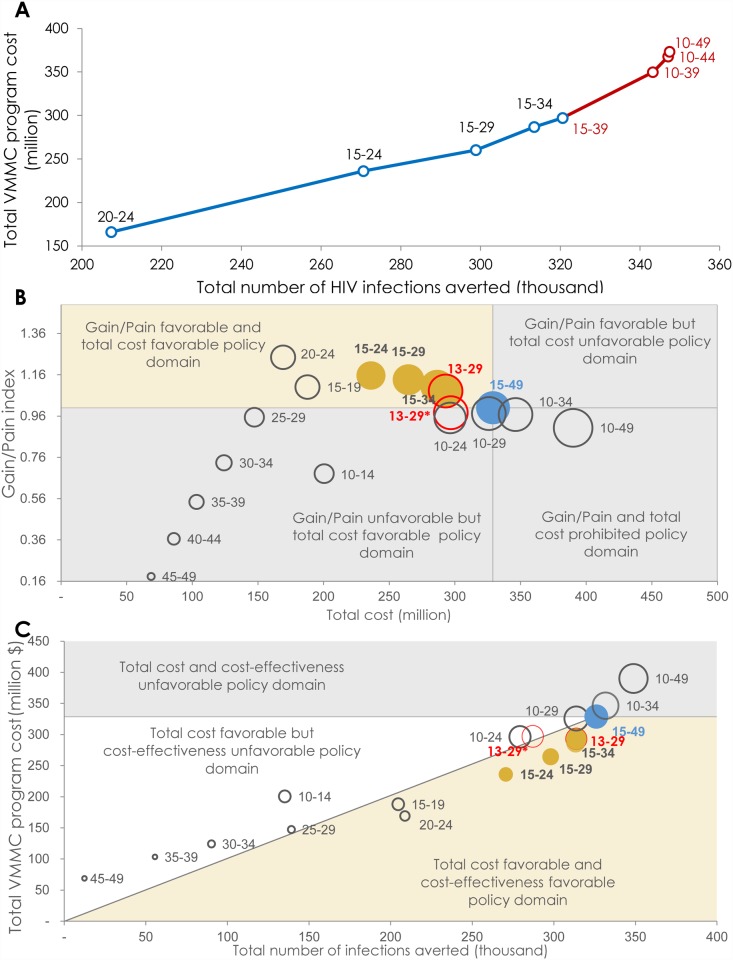
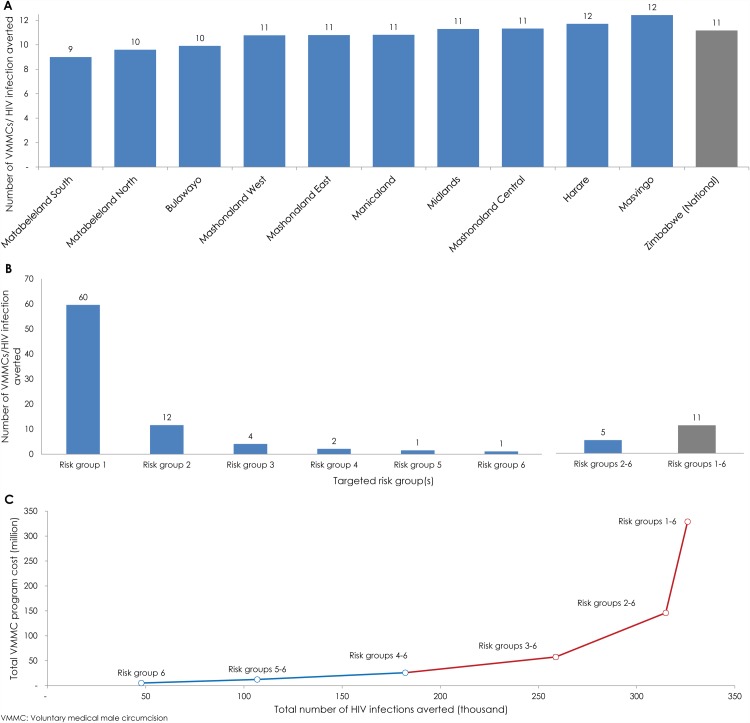
We implemented a recently developed analytical approach: the age-structured mathematical (ASM) model and accompanying three-level conceptual framework to assess the impact of VMMC as an intervention. By September 2014, 364,185 males were circumcised, an initiative that is estimated to avert 40,301 HIV infections by 2025. Through age-group prioritization, the number of VMMCs needed to avert one infection (effectiveness) ranged between ten (20-24 age-group) and 53 (45-49 age-group). The cost per infection averted ranged between $811 (20-24 age-group) and $5,518 (45-49 age-group). By 2025, the largest reductions in HIV incidence rate (up to 27%) were achieved by prioritizing 10-14, 15-19, or 20-24 year old. The greatest program efficiency was achieved by prioritizing 15-24, 15-29, or 15-34 year old. Prioritizing males 13-29 year old was programmatically efficient, but slightly inferior to the 15-24, 15-29, or 15-34 age groups. Through geographic prioritization, effectiveness varied from 9-12 VMMCs per infection averted across provinces. Through risk-group prioritization, effectiveness ranged from one (highest sexual risk-group) to 60 (lowest sexual risk-group) VMMCs per infection averted.
The current VMMC program plan in Zimbabwe is targeting an efficient and impactful age bracket (13-29 year old), but program efficiency can be improved by prioritizing a subset of males for demand creation and service availability. The greatest program efficiency can be attained by prioritizing young sexually active males and males whose sexual behavior puts them at higher risk for acquiring HIV.
津巴布韦的自愿男性包皮环切术(VMMC)项目旨在到2017年时为80%的13至29岁男性进行包皮环切。我们评估了迄今为止VMMC实际推广的影响,并通过对亚人群进行优先排序来评估对该项目进行潜在调整以提高项目效率的影响。
我们采用了一种最近开发的分析方法:年龄结构数学(ASM)模型及配套的三级概念框架,以评估VMMC作为一种干预措施的影响。截至2014年9月,已有364,185名男性接受了包皮环切,据估计这一举措到2025年可避免40,301例HIV感染。通过按年龄组进行优先排序,避免一例感染所需的VMMC数量(有效性)在10例(20 - 24岁年龄组)至53例(45 - 49岁年龄组)之间。避免一例感染的成本在811美元(20 - 24岁年龄组)至5,518美元(45 - 49岁年龄组)之间。到2025年,通过对10 - 14岁、15 - 19岁或20 - 24岁年龄组进行优先排序,HIV发病率的最大降幅(高达27%)得以实现。通过对15 - 24岁、15 - 29岁或15 - 34岁年龄组进行优先排序,实现了最高的项目效率。对13 - 29岁男性进行优先排序在项目实施上是有效的,但略逊于15 - 24岁、15 - 29岁或15 - 34岁年龄组。通过按地理区域进行优先排序,各省每避免一例感染所需的VMMC数量在9至12例之间。通过按风险组进行优先排序,每避免一例感染所需的VMMC数量从1例(性风险最高组)到60例(性风险最低组)不等。
津巴布韦目前的VMMC项目计划针对的是一个高效且有影响力的年龄组(13 - 29岁),但通过对一部分男性进行优先排序以创造需求和提供服务,可以提高项目效率。通过对性活跃年轻男性以及性行为使其感染HIV风险较高的男性进行优先排序,可实现最高的项目效率。