Kripke Katharine, Perales Nicole, Lija Jackson, Fimbo Bennet, Mlanga Eric, Mahler Hally, Juma James McOllogi, Baingana Emmanuel, Plotkin Marya, Kakiziba Deogratias, Semini Iris, Castor Delivette, Njeuhmeli Emmanuel
Health Policy Project, Avenir Health, Glastonbury, Connecticut, United States of America.
Health Policy Project, Futures Group, Washington, District of Columbia, United States of America.
PLoS One. 2016 Jul 13;11(7):e0153363. doi: 10.1371/journal.pone.0153363. eCollection 2016.
Since its launch in 2010, the Tanzania National Voluntary Medical Male Circumcision (VMMC) Program has focused efforts on males ages 10-34 in 11 priority regions. Implementers have noted that over 70% of VMMC clients are between the ages of 10 and 19, raising questions about whether additional efforts would be required to recruit men age 20 and above. This analysis uses mathematical modeling to examine the economic and epidemiological consequences of scaling up VMMC among specific age groups and priority regions in Tanzania.
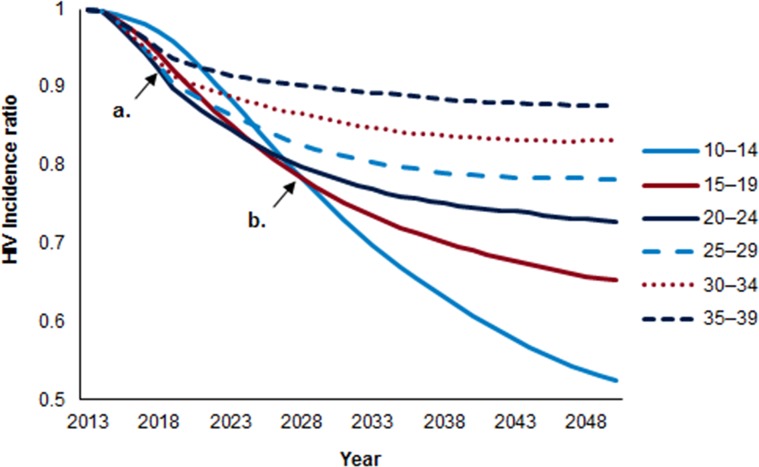
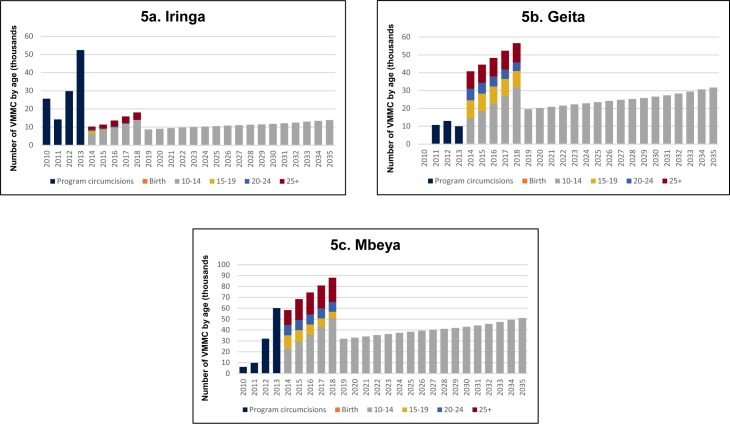
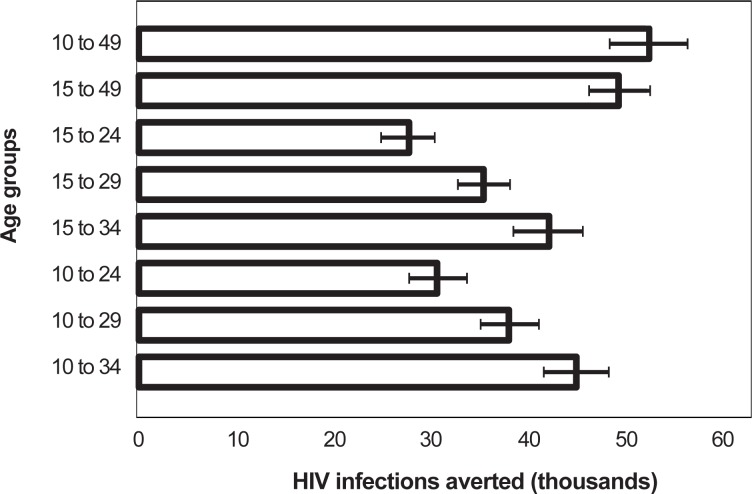
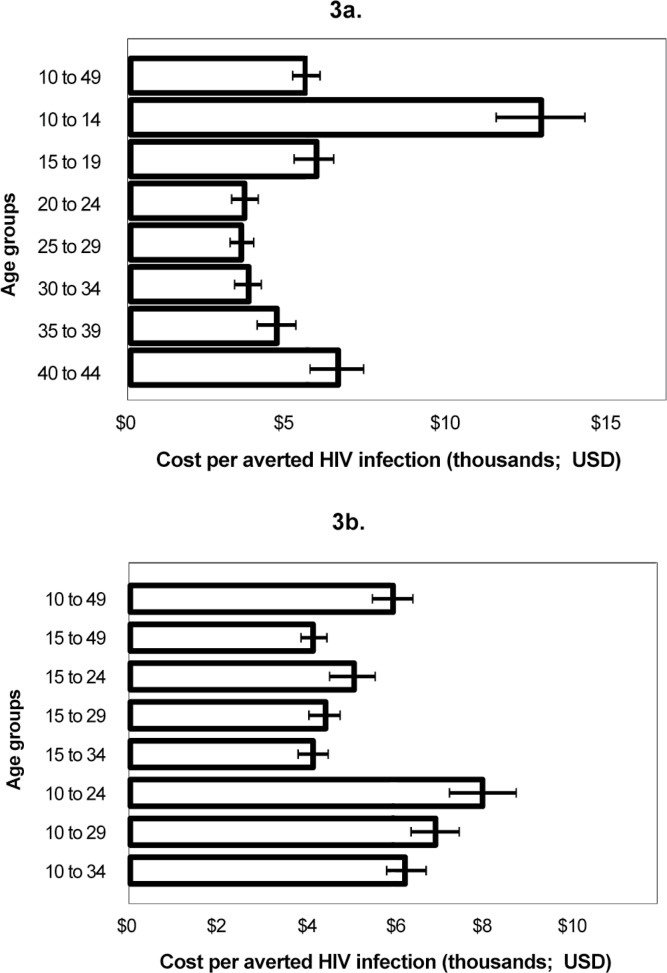
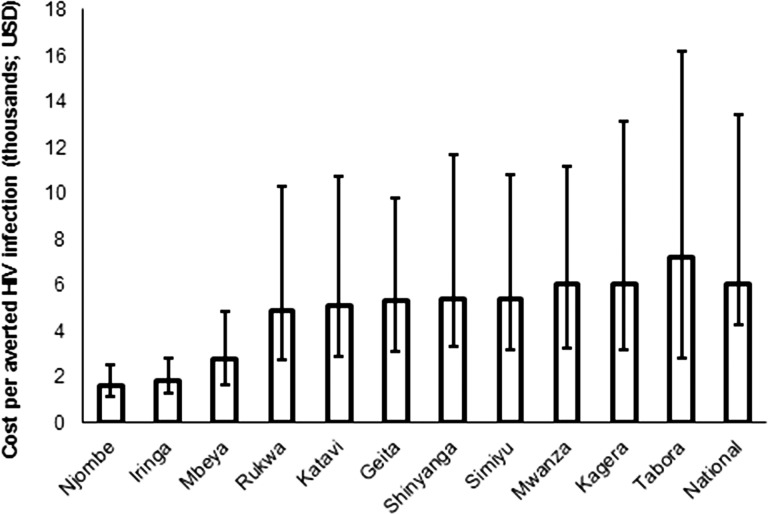
Analyses were conducted using the Decision Makers' Program Planning Tool Version 2.0 (DMPPT 2.0), a compartmental model implemented in Microsoft Excel 2010. The model was populated with population, mortality, and HIV incidence and prevalence projections from external sources, including outputs from Spectrum/AIDS Impact Module (AIM). A separate DMPPT 2.0 model was created for each of the 11 priority regions. Tanzania can achieve the most immediate impact on HIV incidence by circumcising males ages 20-34. This strategy would also require the fewest VMMCs for each HIV infection averted. Circumcising men ages 10-24 will have the greatest impact on HIV incidence over a 15-year period. The most cost-effective approach (lowest cost per HIV infection averted) targets men ages 15-34. The model shows the VMMC program is cost saving in all 11 priority regions. VMMC program cost-effectiveness varies across regions due to differences in projected HIV incidence, with the most cost-effective programs in Njombe and Iringa.
The DMPPT 2.0 results reinforce Tanzania's current VMMC strategy, providing newfound confidence in investing in circumcising adolescents. Tanzanian policy makers and program implementers will continue to focus scale-up of VMMC on men ages 10-34 years, seeking to maximize program impact and cost-effectiveness while acknowledging trends in demand among the younger and older age groups.
自2010年启动以来,坦桑尼亚国家自愿男性包皮环切术(VMMC)项目一直将工作重点放在11个优先地区的10至34岁男性身上。实施者注意到,超过70%的VMMC服务对象年龄在10至19岁之间,这引发了一个问题,即是否需要做出额外努力来招募20岁及以上的男性。本分析使用数学模型来研究在坦桑尼亚特定年龄组和优先地区扩大VMMC的经济和流行病学后果。
使用决策者项目规划工具版本2.0(DMPPT 2.0)进行分析,这是一个在Microsoft Excel 2010中实现的 compartments模型。该模型使用了来自外部来源的人口、死亡率以及艾滋病毒发病率和流行率预测数据,包括Spectrum/艾滋病影响模块(AIM)的输出结果。为11个优先地区中的每个地区创建了一个单独的DMPPT 2.0模型。通过对20至34岁男性进行包皮环切术,坦桑尼亚能够对艾滋病毒发病率产生最直接的影响。该策略每避免一例艾滋病毒感染所需的VMMC手术数量也最少。在15年期间,对10至24岁男性进行包皮环切术将对艾滋病毒发病率产生最大影响。最具成本效益的方法(每避免一例艾滋病毒感染的成本最低)针对的是15至34岁的男性。该模型显示,VMMC项目在所有11个优先地区都能节省成本。由于预计的艾滋病毒发病率存在差异,VMMC项目的成本效益在不同地区有所不同,Njombe和Iringa的项目成本效益最高。
DMPPT 2.0的结果强化了坦桑尼亚目前的VMMC策略,为投资于青少年包皮环切术提供了新的信心。坦桑尼亚政策制定者和项目实施者将继续把VMMC的扩大重点放在10至34岁的男性身上,在认识到年轻和年长年龄组需求趋势的同时,力求使项目影响和成本效益最大化。