Kripke Katharine, Chimbwandira Frank, Mwandi Zebedee, Matchere Faustin, Schnure Melissa, Reed Jason, Castor Delivette, Sgaier Sema, Njeuhmeli Emmanuel
Health Policy Project, Avenir Health, Washington, DC, United States of America.
Ministry of Health, Lilongwe, Malawi.
PLoS One. 2016 Jul 13;11(7):e0156521. doi: 10.1371/journal.pone.0156521. eCollection 2016.
In 2007, the World Health Organization (WHO) recommended scaling up voluntary medical male circumcision (VMMC) in priority countries with high HIV prevalence and low male circumcision (MC) prevalence. According to the Joint United Nations Programme on HIV/AIDS (UNAIDS), an estimated 5.8 million males had undergone VMMC by the end of 2013. Implementation experience has raised questions about the need to refocus VMMC programs on specific subpopulations for the greatest epidemiological impact and programmatic effectiveness. As Malawi prepared its national operational plan for VMMC, it sought to examine the impacts of focusing on specific subpopulations by age and region.
We used the Decision Makers' Program Planning Toolkit, Version 2.0, to study the impact of scaling up VMMC to different target populations of Malawi. National MC prevalence by age group from the 2010 Demographic and Health Survey was scaled according to the MC prevalence for each district and then halved, to adjust for over-reporting of circumcision. In-country stakeholders advised a VMMC unit cost of $100, based on implementation experience. We derived a cost of $451 per patient-year for antiretroviral therapy from costs collected as part of a strategic planning exercise previously conducted in- country by UNAIDS.
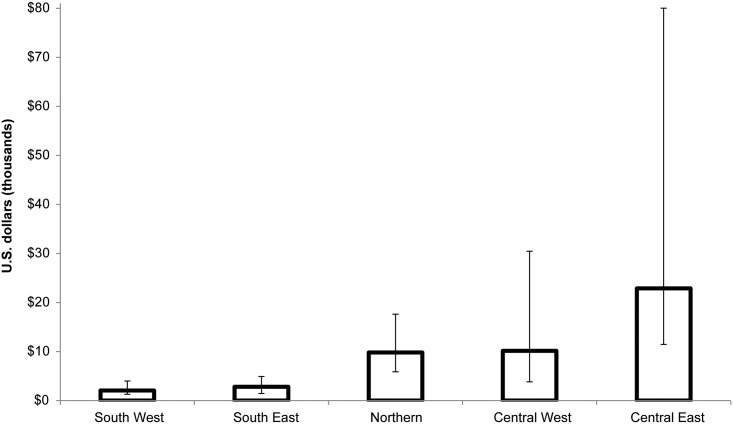
Over a fifteen-year period, circumcising males ages 10-29 would avert 75% of HIV infections, and circumcising males ages 10-34 would avert 88% of infections, compared to the current strategy of circumcising males ages 15-49. The Ministry of Health's South West and South East health zones had the lowest cost per HIV infection averted. Moreover, VMMC met WHO's definition of cost-effectiveness (that is, the cost per disability-adjusted life-year [DALY] saved was less than three times the per capita gross domestic product) in all health zones except Central East. Comparing urban versus rural areas in the country, we found that circumcising men in urban areas would be both cost-effective and cost-saving, with a VMMC cost per DALY saved of $120 USD and with 15 years of VMMC implementation resulting in lifetime HIV treatment costs savings of $331 million USD.
Based on the age analyses and programmatic experience, Malawi's VMMC operational plan focuses on males ages 10-34 in all districts in the South East and South West zones, as well as Lilongwe (an urban district in the Central zone). This plan covers 14 of the 28 districts in the country.
2007年,世界卫生组织(WHO)建议在艾滋病毒高流行率和低男性包皮环切术(MC)流行率的优先国家扩大自愿男性包皮环切术(VMMC)。根据联合国艾滋病毒/艾滋病联合规划署(UNAIDS)的数据,到2013年底,估计有580万男性接受了VMMC。实施经验引发了关于是否需要将VMMC项目重新聚焦于特定亚人群以实现最大流行病学影响和项目有效性的问题。马拉维在制定其国家VMMC业务计划时,试图研究按年龄和地区聚焦特定亚人群的影响。
我们使用决策制定者项目规划工具包2.0来研究扩大VMMC规模对马拉维不同目标人群的影响。根据2010年人口与健康调查按年龄组划分的全国MC流行率,按照每个地区的MC流行率进行调整,然后减半,以调整包皮环切术报告过高的情况。根据实施经验,国内利益相关者建议VMMC单位成本为100美元。我们从UNAIDS此前在该国进行的一项战略规划活动收集的成本中得出抗逆转录病毒疗法每位患者每年的成本为451美元。
在15年期间,与目前对15 - 49岁男性进行包皮环切术的策略相比,对10 - 29岁男性进行包皮环切术可避免75%的艾滋病毒感染,对10 - 34岁男性进行包皮环切术可避免88%的感染。卫生部的西南和东南卫生区避免每例艾滋病毒感染的成本最低。此外,除中东外,VMMC在所有卫生区都符合世卫组织的成本效益定义(即每挽救一个伤残调整生命年[DALY]的成本低于人均国内生产总值的三倍)。比较该国城乡地区,我们发现对城市男性进行包皮环切术既具有成本效益又能节省成本,每挽救一个DALY的VMMC成本为120美元,实施15年的VMMC可节省3.31亿美元的终身艾滋病毒治疗成本。
基于年龄分析和项目经验,马拉维的VMMC业务计划聚焦于东南和西南区所有地区以及利隆圭(中区的一个城市区)的10 - 34岁男性。该计划覆盖该国28个区中的14个。