Division of Orthopaedic Surgery, Department of Surgery, McMaster University, Hamilton, Ontario, Canada.
Division of Orthopaedics, Department of Surgery, St. Michael's Hospital, Toronto, Ontario, Canada.
Orthop J Sports Med. 2014 Jul 21;2(7):2325967114541414. doi: 10.1177/2325967114541414. eCollection 2014 Jul.
A diagnosis of femoroacetabular impingement (FAI) requires careful history and physical examination, as well as an accurate and reliable radiologic evaluation using plain radiographs as a screening modality. Radiographic markers in the diagnosis of FAI are numerous and not fully validated. In particular, reliability in their assessment across health care providers is unclear.
To determine inter- and intraobserver reliability between orthopaedic surgeons and musculoskeletal radiologists.
Cohort study (diagnosis); Level of evidence, 3.
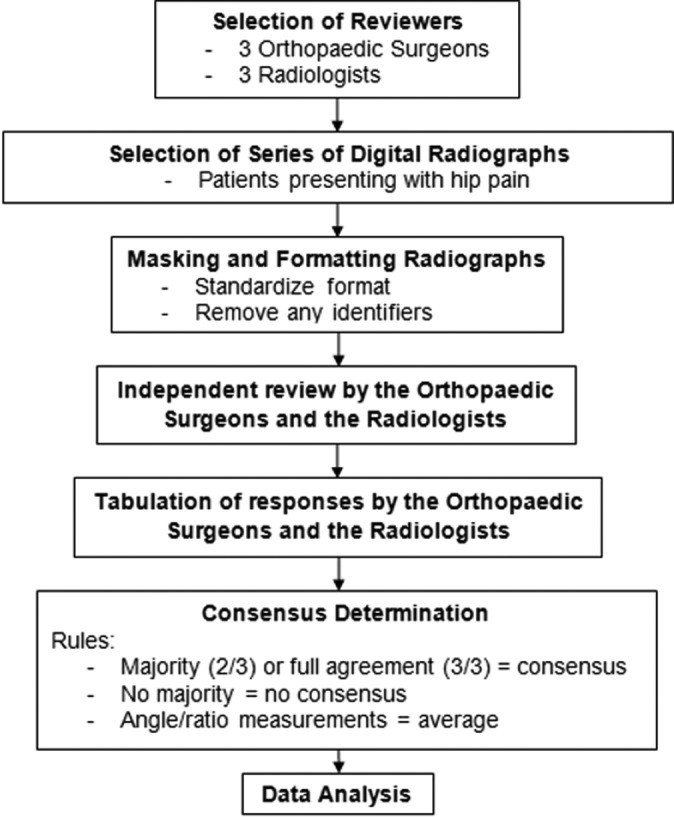
Six physicians (3 orthopaedic surgeons, 3 musculoskeletal radiologists) independently evaluated a broad spectrum of FAI pathologies across 51 hip radiographs on 2 occasions separated by at least 4 weeks. Reviewers used 8 common criteria to diagnose FAI, including (1) pistol-grip deformity, (2) size of alpha angle, (3) femoral head-neck offset, (4) posterior wall sign abnormality, (5) ischial spine sign abnormality, (6) coxa profunda abnormality, (7) crossover sign abnormality, and (8) acetabular protrusion. Agreement was calculated using the intraclass correlation coefficient (ICC).
When establishing an FAI diagnosis, there was poor interobserver reliability between the surgeons and radiologists (ICC batch 1 = 0.33; ICC batch 2 = 0.15). In contrast, there was higher interobserver reliability within each specialty, ranging from fair to good (surgeons: ICC batch 1 = 0.72; ICC batch 2 = 0.70 vs radiologists: ICC batch 1 = 0.59; ICC batch 2 = 0.74). Orthopaedic surgeons had the highest interobserver reliability when identifying pistol-grip deformities (ICC = 0.81) or abnormal alpha angles (ICC = 0.81). Similarly, radiologists had the highest agreement for detecting pistol-grip deformities (ICC = 0.75).
These results suggest that surgeons and radiologists agree among themselves, but there is a need to improve the reliability of radiographic interpretations for FAI between the 2 specialties. The observed degree of low reliability may ultimately lead to missed, delayed, or inappropriate treatments for patients with symptomatic FAI.
髋关节撞击综合征(FAI)的诊断需要仔细的病史和体格检查,以及使用平片作为筛查手段的准确可靠的影像学评估。FAI 诊断中的影像学标志物很多,但尚未完全得到验证。特别是,不同医疗服务提供者对其评估的可靠性尚不清楚。
确定骨科医生和肌肉骨骼放射科医生之间的组内和组间可靠性。
队列研究(诊断);证据水平,3 级。
6 名医生(3 名骨科医生,3 名肌肉骨骼放射科医生)在至少 4 周的 2 次评估中,分别独立评估了 51 张髋关节 X 线片上的广泛 FAI 病变。评估者使用 8 种常见标准来诊断 FAI,包括(1)手枪握畸形,(2)α角大小,(3)股骨头颈偏移,(4)后侧壁征异常,(5)坐骨棘征异常,(6)髋深畸形,(7)交叉征异常,和(8)髋臼突出。使用组内相关系数(ICC)计算一致性。
当建立 FAI 诊断时,外科医生和放射科医生之间的组间一致性较差(ICC 批次 1=0.33;ICC 批次 2=0.15)。相比之下,每个专业内部的组间一致性更高,范围从一般到良好(外科医生:ICC 批次 1=0.72;ICC 批次 2=0.70 与放射科医生:ICC 批次 1=0.59;ICC 批次 2=0.74)。当识别手枪握畸形(ICC=0.81)或异常α角(ICC=0.81)时,骨科医生具有最高的组间一致性。同样,放射科医生在检测手枪握畸形时具有最高的一致性(ICC=0.75)。
这些结果表明,外科医生和放射科医生彼此之间存在一致性,但需要提高这两个专业之间对 FAI 的影像学解释的可靠性。观察到的低可靠性程度可能最终导致对有症状 FAI 患者的漏诊、延误或不适当治疗。