Guthrie Bruce, Donnan Peter T, Murphy Douglas J, Makubate Boikanyo, Dreischulte Tobias
Quality, Safety and Informatics Research Group, Population Health Sciences Division, Medical Research Institute, University of Dundee, Mackenzie Building, Kirsty Semple Way, Dundee, UK.
Dundee Epidemiology and Biostatistics Unit, Population Health Sciences Division, Medical Research Institute, University of Dundee, Mackenzie Building, Kirsty Semple Way, Dundee, UK.
BMJ Open. 2015 Nov 6;5(11):e008270. doi: 10.1136/bmjopen-2015-008270.
Primary care high-risk prescribing causes significant harm, but it is unclear if it is largely driven by individuals (a 'bad apple' problem) or by practices having higher or lower risk prescribing cultures (a 'spoiled barrel' problem). The study aimed to examine the extent of variation in high-risk prescribing between individual prescribers and between the practices they work in.
DESIGN, SETTING AND PARTICIPANTS: Multilevel logistic regression modelling of routine cross-sectional data from 38 Scottish general practices for 181,010 encounters between 398 general practitioners (GPs) and 26,539 patients particularly vulnerable to adverse drug events (ADEs) of non-steroidal anti-inflammatory drugs (NSAIDs) due to age, comorbidity or co-prescribing.
Initiation of a new NSAID prescription in an encounter between GPs and eligible patients.
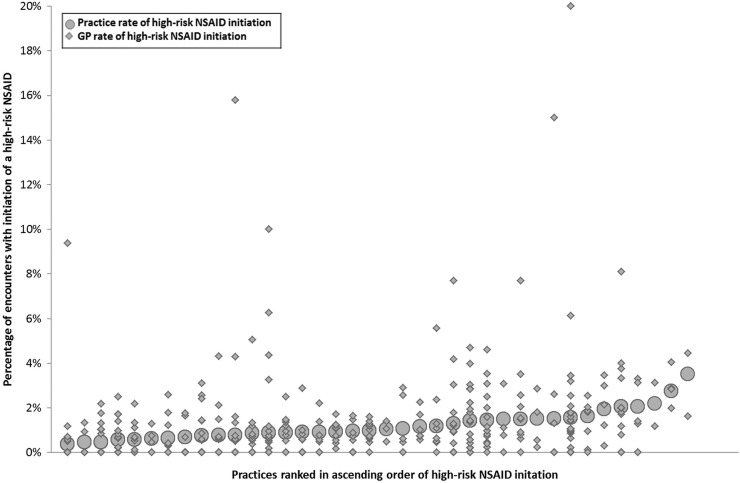
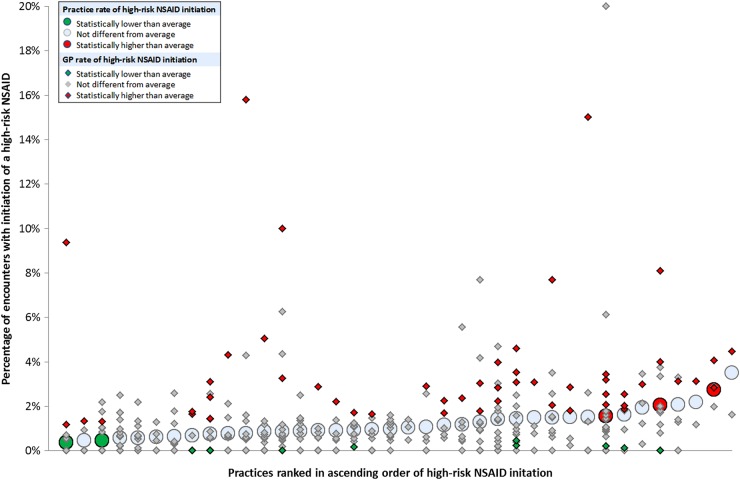
A new high-risk NSAID was initiated in 1953 encounters (1.1% of encounters, 7.4% of patients). Older patients, those with more vulnerabilities to NSAID ADEs and those with polypharmacy were less likely to have a high-risk NSAID initiated, consistent with GPs generally recognising the risk of NSAIDs in eligible patients. Male GPs were more likely to initiate a high-risk NSAID than female GPs (OR 1.73, 95% CI 1.39 to 2.16). After accounting for patient characteristics, 4.2% (95% CI 2.1 to 8.3) of the variation in high-risk NSAID prescribing was attributable to variation between practices, and 14.2% (95% CI 11.4 to 17.3) to variation between GPs. Three practices had statistically higher than average high-risk prescribing, but only 15.7% of GPs with higher than average high-risk prescribing and 18.5% of patients receiving such a prescription were in these practices.
There was much more variation in high-risk prescribing between GPs than between practices, and only targeting practices with higher than average rates will miss most high-risk NSAID prescribing. Primary care prescribing safety improvement should ideally target all practices, but encourage practices to consider and act on variation between prescribers in the practice.
基层医疗中的高风险处方会造成重大危害,但尚不清楚这主要是由个体因素(“坏苹果”问题)导致,还是由具有高低不同风险处方文化的医疗机构造成(“坏桶”问题)。本研究旨在调查个体开处方者之间以及他们所在医疗机构之间高风险处方的差异程度。
设计、背景与参与者:对来自苏格兰38家全科医疗诊所的常规横断面数据进行多水平逻辑回归建模,涉及398名全科医生(GP)与26539名患者之间的181010次诊疗,这些患者因年龄、合并症或联合用药等因素,特别容易发生非甾体抗炎药(NSAID)的药物不良事件(ADE)。
在全科医生与符合条件的患者诊疗过程中开具新的NSAID处方。
在1953次诊疗中开具了新的高风险NSAID处方(占诊疗次数的1.1%,患者的7.4%)。老年患者、更容易发生NSAID ADE的患者以及服用多种药物的患者开具高风险NSAID处方的可能性较小,这与全科医生普遍认识到符合条件患者使用NSAID的风险一致。男性全科医生比女性全科医生更有可能开具高风险NSAID处方(比值比1.73,95%置信区间1.39至2.16)。在考虑患者特征后,高风险NSAID处方差异的4.2%(95%置信区间2.1至8.3)可归因于不同诊所之间的差异,14.2%(95%置信区间11.4至17.3)可归因于全科医生之间的差异。有三家诊所的高风险处方在统计学上高于平均水平,但高风险处方高于平均水平的全科医生中只有15.7%,接受此类处方的患者中只有18.5%在这些诊所。
全科医生之间高风险处方的差异远大于诊所之间的差异,仅针对高于平均水平的诊所将遗漏大多数高风险NSAID处方。基层医疗处方安全性的改善理想情况下应针对所有诊所,但鼓励诊所考虑并应对诊所内开处方者之间的差异并采取行动。