Abe Mitsuhiro, Tsushima Kenji, Matsumura Takuma, Ishiwata Tsukasa, Ichimura Yasunori, Ikari Jun, Terada Jiro, Tada Yuji, Sakao Seiichirou, Tanabe Nobuhiro, Tatsumi Koichiro
Department of Respirology, Graduate School of Medicine, Chiba University, Chiba, Japan.
Drug Des Devel Ther. 2015 Oct 23;9:5755-62. doi: 10.2147/DDDT.S90739. eCollection 2015.
Acute exacerbation (AE) is an important outcome of idiopathic pulmonary fibrosis (IPF) and nonspecific interstitial pneumonia (NSIP). Recombinant human soluble thrombomodulin (rhTM) is a new drug for the treatment of disseminated intravascular coagulation in Japan. The objective of this study was to evaluate the efficacy of rhTM for AE of IPF/NSIP.
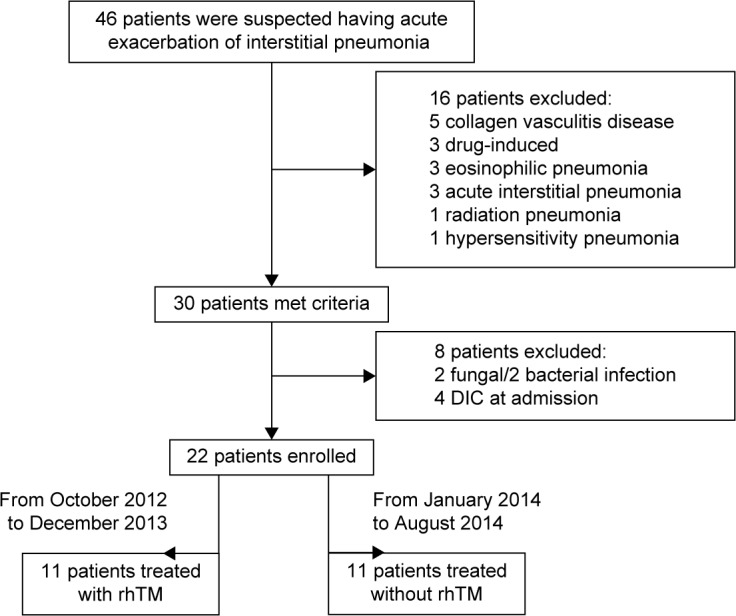
Twenty-two patients with AE-idiopathic interstitial pneumonia (16 patients with IPF and six patients with NSIP) were enrolled in our study. Among them, eleven patients were treated with rhTM (rhTM group), and eleven patients were treated without rhTM (non-rhTM group). Patients admitted to our hospital prior to December 2013 were treated with rhTM, while those admitted after January 2014 were treated without rhTM. The primary endpoint was mortality at 90 days after AE treatment. The secondary endpoint was the safety of rhTM for AE-IPF/AE-NSIP. In addition, we examined prognostic factors of AE-IPF/AE-NSIP.
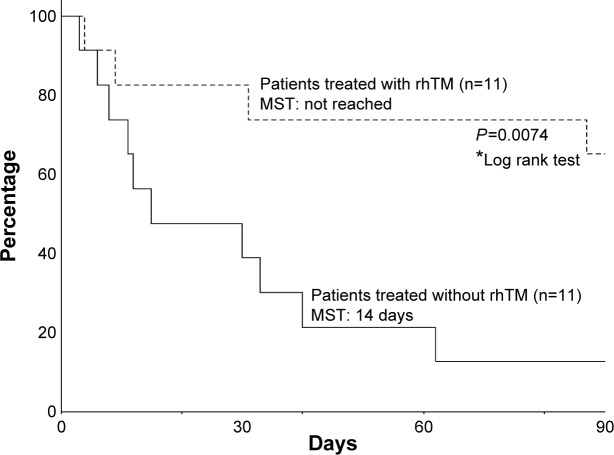
The mortality rate was significantly lower in the rhTM group than in the non-rhTM group (mortality rate at 90 days: 36% vs 90%, P=0.023; median survival time: not reached vs 15.0 days, P=0.019). A univariate analysis revealed the respiratory rate (hazard ratio [HR] 1.09, 95% confidence interval [CI] 1.00-1.18, P=0.039) and rhTM administration (HR 0.21, 95% CI 0.06-0.77, P=0.013) as predictors of mortality at 90 days, and a multivariate analysis identified rhTM administration (HR 0.025, 95% CI 0.0006-0.94, P=0.046) as an independent predictor of mortality at 90 days. No serious adverse events were observed.
The administration of rhTM is associated with reductions in mortality in patients with AE-IPF/NSIP, without causing adverse events.
急性加重(AE)是特发性肺纤维化(IPF)和非特异性间质性肺炎(NSIP)的一项重要结局。重组人可溶性血栓调节蛋白(rhTM)在日本是一种用于治疗弥散性血管内凝血的新药。本研究的目的是评估rhTM对IPF/NSIP急性加重的疗效。
22例急性加重期特发性间质性肺炎患者(16例IPF患者和6例NSIP患者)纳入本研究。其中,11例患者接受rhTM治疗(rhTM组),11例患者未接受rhTM治疗(非rhTM组)。2013年12月之前入院的患者接受rhTM治疗,而2014年1月之后入院的患者未接受rhTM治疗。主要终点是AE治疗后90天的死亡率。次要终点是rhTM对AE-IPF/AE-NSIP的安全性。此外,我们研究了AE-IPF/AE-NSIP的预后因素。
rhTM组的死亡率显著低于非rhTM组(90天死亡率:36%对90%,P=0.023;中位生存时间:未达到对15.0天,P=0.019)。单因素分析显示呼吸频率(风险比[HR]1.09,95%置信区间[CI]1.00-1.18,P=0.039)和rhTM给药(HR 0.21,95%CI 0.06-0.77,P=0.013)是90天死亡率的预测因素,多因素分析确定rhTM给药(HR 0.025,95%CI 0.0006-0.94,P=0.046)是90天死亡率的独立预测因素。未观察到严重不良事件。
rhTM给药与AE-IPF/NSIP患者死亡率降低相关,且未引起不良事件。