Harvey J, Dopson S, McManus R J, Powell J
Nuffield Department of Primary Care Health Sciences, University of Oxford, Radcliffe Observatory Quarter, Woodstock road, Oxford, OX2 6GG, UK.
Saïd Business School, University of Oxford, Park End Street, Oxford, OX1 1HP, UK.
Implement Sci. 2015 Nov 13;10:159. doi: 10.1186/s13012-015-0350-x.
In a research context, self-management solutions, which may range from simple book diaries to complex telehealth packages, designed to facilitate patients in managing their long-term conditions, have often shown cost-effectiveness, but their implementation in practice has frequently been challenging.
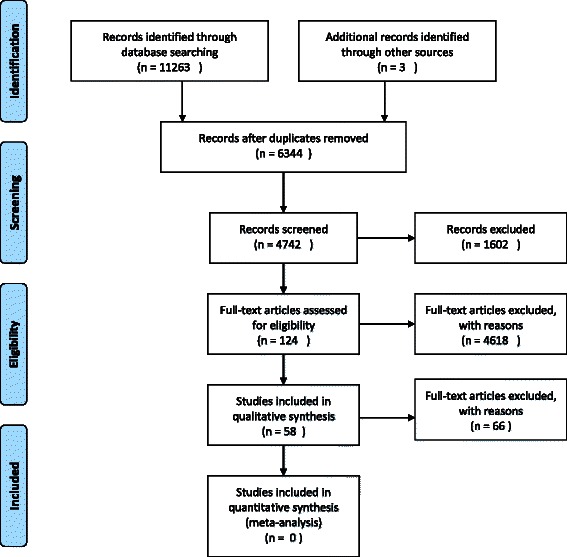
We conducted an interpretive qualitative synthesis of relevant articles identified through systematic searches of bibliographic databases in July 2014. We searched PubMed (Medline/NLM), Web of Science, LISTA (EBSCO), CINAHL, Embase and PsycINFO. Coding and analysis was inductive, using the framework method to code and to categorise themes. We took a sensemaking approach to the interpretation of findings.
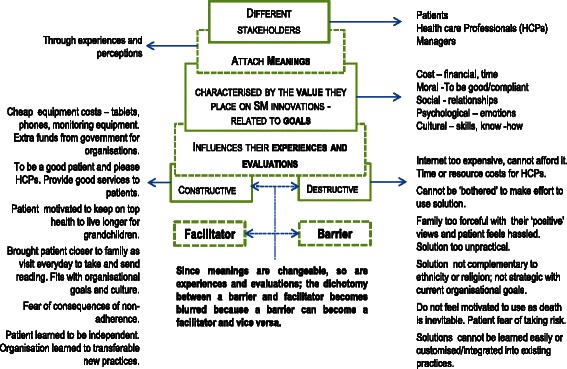
Fifty-eight articles were selected for synthesis. Results showed that during adoption, factors identified as facilitators by some were experienced as barriers by others, and facilitators could change to barriers for the same adopter, depending on how adopters rationalise the solutions within their context when making decisions about (retaining) adoption. Sometimes, when adopters saw and experienced benefits of a solution, they continued using the solution but changed their minds when they could no longer see the benefits. Thus, adopters placed a positive value on the solution if they could constructively rationalise it (which increased adoption) and attached a negative rationale (decreasing adoption) if the solution did not meet their expectations. Key factors that influenced the way adopters rationalised the solutions consisted of costs and the added value of the solution to them and moral, social, motivational and cultural factors.
Considering 'barriers' and 'facilitators' for implementation may be too simplistic. Implementers could instead iteratively re-evaluate how potential facilitators and barriers are being experienced by adopters throughout the implementation process, to help adopters to retain constructive evaluations of the solution. Implementers need to pay attention to factors including (a) cost: how much resource will the intervention cost the patient or professional; (b) moral: to what extent will people adhere because they want to be 'good' patients and professionals; (c) social: the expectations of patients and professionals regarding the interactive support they will receive; (d) motivational: motivations to engage with the intervention and (e) cultural: how patients and professionals learn and integrate new skills into their daily routines, practices and cultures.
在研究背景下,自我管理解决方案,其范围可能从简单的纸质日记到复杂的远程医疗套餐,旨在帮助患者管理其长期疾病,这些方案常常显示出成本效益,但在实际应用中实施起来却常常具有挑战性。
我们对通过2014年7月对书目数据库进行系统检索而确定的相关文章进行了诠释性定性综合分析。我们检索了PubMed(Medline/美国国立医学图书馆)、科学引文索引、LISTA(EBSCO)、护理学与健康领域数据库、Embase和心理学文摘数据库。编码和分析采用归纳法,使用框架方法对主题进行编码和分类。我们采用了一种意义建构的方法来解释研究结果。
选取了58篇文章进行综合分析。结果表明,在采用过程中,一些人认为是促进因素的因素,另一些人却将其视为障碍,而且对于同一采用者来说,促进因素可能会转变为障碍,这取决于采用者在做出(保留)采用决定时如何在其背景下对解决方案进行合理化解释。有时,当采用者看到并体验到一种解决方案的益处时,他们会继续使用该方案,但当他们再也看不到益处时就会改变主意。因此,如果采用者能够建设性地对解决方案进行合理化解释(这会增加采用率),他们就会对该解决方案给予积极评价;如果该解决方案不符合他们的期望,他们就会给出负面的理由(降低采用率)。影响采用者对解决方案进行合理化解释方式的关键因素包括成本、解决方案对他们的附加值以及道德、社会、动机和文化因素。
考虑实施过程中的“障碍”和“促进因素”可能过于简单化。实施者可以改为在整个实施过程中反复重新评估采用者如何体验潜在的促进因素和障碍,以帮助采用者对解决方案保持建设性的评价。实施者需要关注以下因素:(a)成本:该干预措施将使患者或专业人员花费多少资源;(b)道德:人们在多大程度上会因为想成为“好”患者和专业人员而坚持;(c)社会:患者和专业人员对他们将获得的互动支持的期望;(d)动机:参与干预的动机;(e)文化:患者和专业人员如何学习并将新技能融入他们的日常生活、实践和文化中。