Rigouts L, Coeck N, Gumusboga M, de Rijk W B, Aung K J M, Hossain M A, Fissette K, Rieder H L, Meehan C J, de Jong B C, Van Deun A
Mycobacteriology Unit, Department of Biomedical Sciences, Institute of Tropical Medicine, Antwerp, Belgium Biomedical Sciences, University of Antwerp, Antwerp, Belgium
Mycobacteriology Unit, Department of Biomedical Sciences, Institute of Tropical Medicine, Antwerp, Belgium Biomedical Sciences, University of Antwerp, Antwerp, Belgium.
J Antimicrob Chemother. 2016 Feb;71(2):314-23. doi: 10.1093/jac/dkv360. Epub 2015 Nov 24.
Mutations in the gyrase genes cause fluoroquinolone resistance in Mycobacterium tuberculosis. However, the predictive value of these markers for clinical outcomes in patients with MDR-TB is unknown to date. The objective of this study was to determine molecular markers and breakpoints predicting second-line treatment outcomes in M. tuberculosis patients treated with fourth-generation fluoroquinolones.
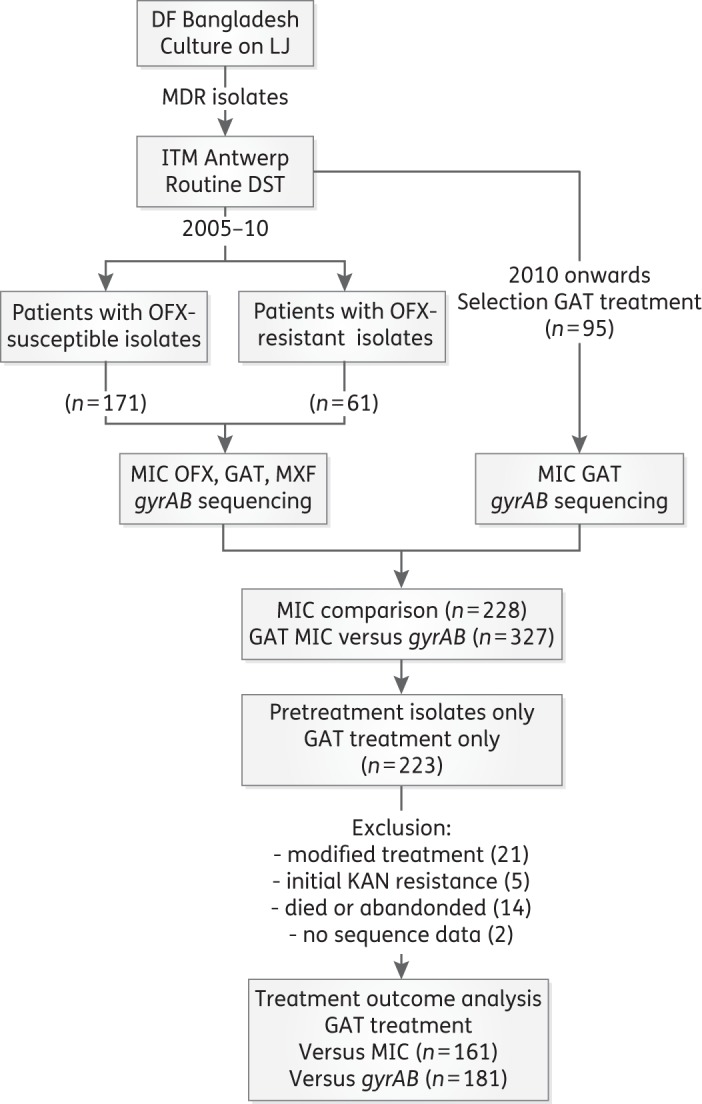
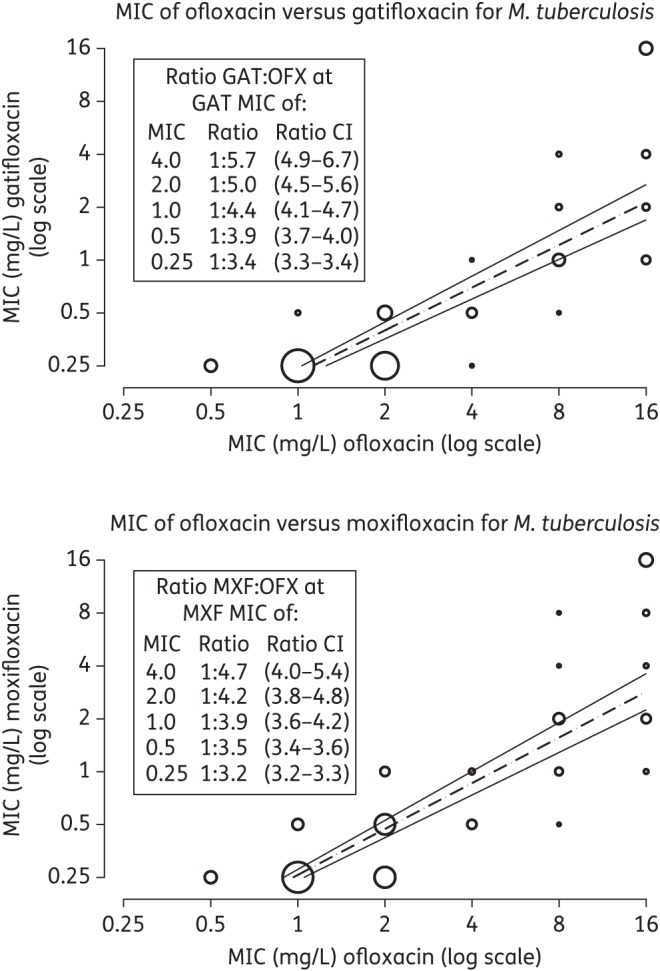
We analysed treatment outcome data in relation to the gyrA and gyrB sequences and MICs of ofloxacin, gatifloxacin and moxifloxacin for pretreatment M. tuberculosis isolates from 181 MDR-TB patients in Bangladesh whose isolates were susceptible to injectable drugs.
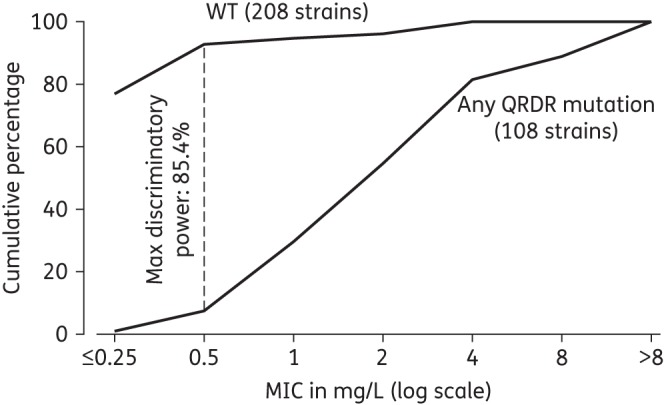
The gyrA 90Val, 94Gly and 94Ala mutations were most frequent, with the highest resistance levels for 94Gly mutants. Increased pretreatment resistance levels (>2 mg/L), related to specific mutations, were associated with lower cure percentages, with no cure in patients whose isolates were resistant to gatifloxacin at 4 mg/L. Any gyrA 94 mutation, except 94Ala, predicted a significantly lower proportion of cure compared with all other gyrA mutations taken together (all non-94 mutants + 94Ala) [OR = 4.3 (95% CI 1.4-13.0)]. The difference in treatment outcome was not explained by resistance to the other drugs.
Our study suggests that gyrA mutations at position 94, other than Ala, predict high-level resistance to gatifloxacin and moxifloxacin, as well as poor treatment outcome, in MDR-TB patients in whom an injectable agent is still effective.
结核分枝杆菌中gyrase基因的突变会导致对氟喹诺酮类药物产生耐药性。然而,迄今为止,这些标志物对耐多药结核病患者临床结局的预测价值尚不清楚。本研究的目的是确定预测接受第四代氟喹诺酮类药物治疗的结核病患者二线治疗结局的分子标志物和断点。
我们分析了来自孟加拉国181例耐多药结核病患者的治疗结局数据,这些患者的结核分枝杆菌分离株对注射用药物敏感,分析内容涉及gyrA和gyrB序列以及氧氟沙星、加替沙星和莫西沙星的最低抑菌浓度(MIC)。
gyrA 90Val、94Gly和94Ala突变最为常见,其中94Gly突变体的耐药水平最高。与特定突变相关的治疗前耐药水平升高(>2mg/L)与治愈率降低相关,分离株对4mg/L加替沙星耐药的患者无治愈病例。与所有其他gyrA突变(所有非94突变体+94Ala)相比,除94Ala外的任何gyrA 94突变预测的治愈比例显著更低[比值比(OR)=4.3(95%置信区间1.4-13.0)]。治疗结局的差异无法用对其他药物的耐药性来解释。
我们的研究表明,在注射用药物仍然有效的耐多药结核病患者中,94位的gyrA突变(非Ala)预示着对加替沙星和莫西沙星的高水平耐药以及不良的治疗结局。