Nankabirwa Joaniter I, Yeka Adoke, Arinaitwe Emmanuel, Kigozi Ruth, Drakeley Chris, Kamya Moses R, Greenhouse Bryan, Rosenthal Philip J, Dorsey Grant, Staedke Sarah G
Department of Medicine, Makerere University College of Health Sciences, Kampala, Uganda.
Infectious Diseases Research Collaboration, Kampala, Uganda.
Malar J. 2015 Dec 30;14:528. doi: 10.1186/s12936-015-1056-x.
Household surveys are important tools for monitoring the malaria disease burden and measuring impact of malaria control interventions with parasite prevalence as the primary metric. However, estimates of parasite prevalence are dependent on a number of factors including the method used to detect parasites, age of the population sampled, and level of immunity. To better understand the influence of diagnostics, age, and endemicity on estimates of parasite prevalence and how these change over time, community-based surveys were performed for two consecutive years in three settings and the sensitivities of microscopy and immunochromatographic rapid diagnostic tests (RDTs) were assessed, considering polymerase chain reaction (PCR) as the gold standard.
Surveys were conducted over the same two-month period in 2012 and 2013 in each of three sub-counties in Uganda: Nagongera in Tororo District (January-February), Walukuba in Jinja District (March-April), and Kihihi in Kanungu District (May-June). In each sub-county, 200 households were randomly enrolled and a household questionnaire capturing information on demographics, use of malaria prevention methods, and proxy indicators of wealth was administered to the head of the household. Finger-prick blood samples were obtained for RDTs, measurement of hemoglobin, thick and thin blood smears, and to store samples on filter paper.
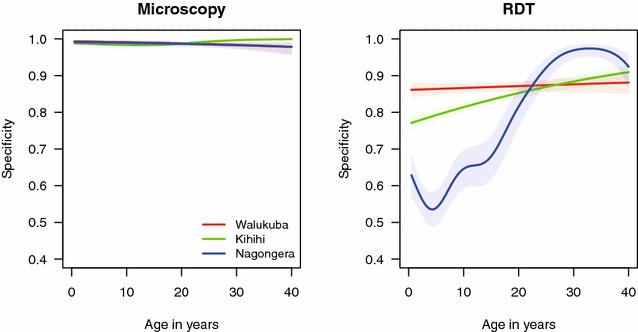
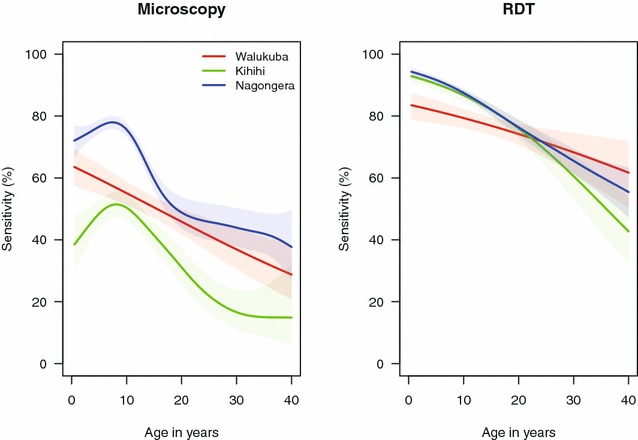
A total of 1200 households were surveyed and 4433 participants were included in the analysis. Compared to PCR, the sensitivity of microscopy was low (65.3% in Nagongera, 49.6% in Walukuba and 40.9% in Kihihi) and decreased with increasing age. The specificity of microscopy was over 98% at all sites and did not vary with age or year. Relative differences in parasite prevalence across different age groups, study sites, and years were similar for microscopy and PCR. The sensitivity of RDTs was similar across the three sites (range 77.2-82.8%), was consistently higher than microscopy (p < 0.001 for all pairwise comparisons), and decreased with increasing age. The specificity of RDTs was lower than microscopy (76.3% in Nagongera, 86.3% in Walukuba, and 83.5% in Kihihi) and varied significantly by year and age. Relative differences in parasite prevalence across age groups and study years differed for RDTs compared to microscopy and PCR.
Malaria prevalence estimates varied with diagnostic test, age, and transmission intensity. It is important to consider the effects of these parameters when designing and interpreting community-based surveys.
家庭调查是监测疟疾疾病负担以及以寄生虫感染率作为主要指标衡量疟疾控制干预措施效果的重要工具。然而,寄生虫感染率的估计取决于多种因素,包括用于检测寄生虫的方法、抽样人群的年龄以及免疫水平。为了更好地理解诊断方法、年龄和地方流行程度对寄生虫感染率估计的影响以及这些因素如何随时间变化,在三个地区连续两年开展了基于社区的调查,并将聚合酶链反应(PCR)作为金标准,评估了显微镜检查和免疫层析快速诊断试验(RDT)的敏感性。
2012年和2013年在乌干达的三个次县的同一两个月期间进行了调查:托罗罗区的纳贡埃拉(1月至2月)、金贾区的瓦卢库巴(3月至4月)以及卡农古区的基希希(5月至6月)。在每个次县,随机选取200户家庭,向户主发放一份家庭问卷,收集有关人口统计学、疟疾预防方法使用情况以及财富替代指标的信息。采集手指刺血样本用于RDT检测、血红蛋白测量、厚薄血涂片检查,并将样本储存在滤纸上。
共调查了1200户家庭,4433名参与者纳入分析。与PCR相比,显微镜检查的敏感性较低(纳贡埃拉为65.3%,瓦卢库巴为49.6%,基希希为40.9%),且随年龄增长而降低。显微镜检查的特异性在所有地点均超过98%,且不随年龄或年份变化。显微镜检查和PCR在不同年龄组、研究地点和年份的寄生虫感染率相对差异相似。RDT在三个地点的敏感性相似(范围为77.2%至82.8%),始终高于显微镜检查(所有成对比较的p<0.001),且随年龄增长而降低。RDT的特异性低于显微镜检查(纳贡埃拉为76.3%,瓦卢库巴为86.3%,基希希为83.5%),且因年份和年龄而有显著差异。与显微镜检查和PCR相比,RDT在不同年龄组和研究年份的寄生虫感染率相对差异不同。
疟疾感染率估计因诊断测试、年龄和传播强度而异。在设计和解释基于社区的调查时,考虑这些参数的影响很重要。