Vanterpool Sizzle F, Been Jasper V, Houben Michiel L, Nikkels Peter G J, De Krijger Ronald R, Zimmermann Luc J I, Kramer Boris W, Progulske-Fox Ann, Reyes Leticia
Department of Pediatrics, Maastricht University Medical Center, Maastricht, the Netherlands.
School for Mental Health and Neurosciences (MHeNS), Maastricht University, Maastricht, the Netherlands.
PLoS One. 2016 Jan 5;11(1):e0146157. doi: 10.1371/journal.pone.0146157. eCollection 2016.
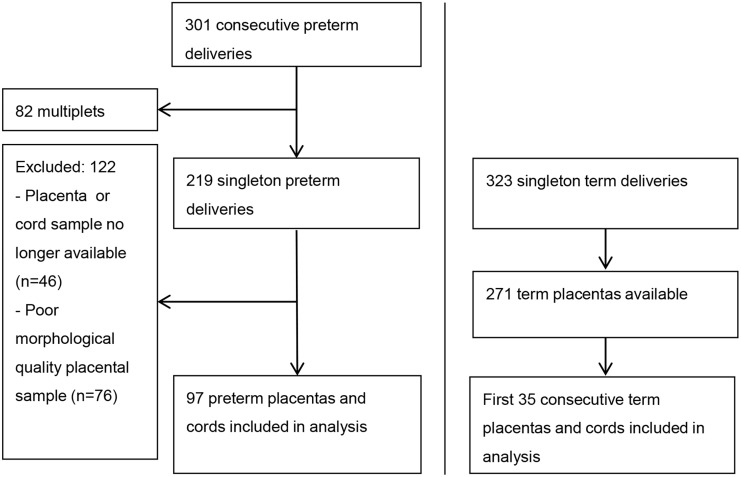
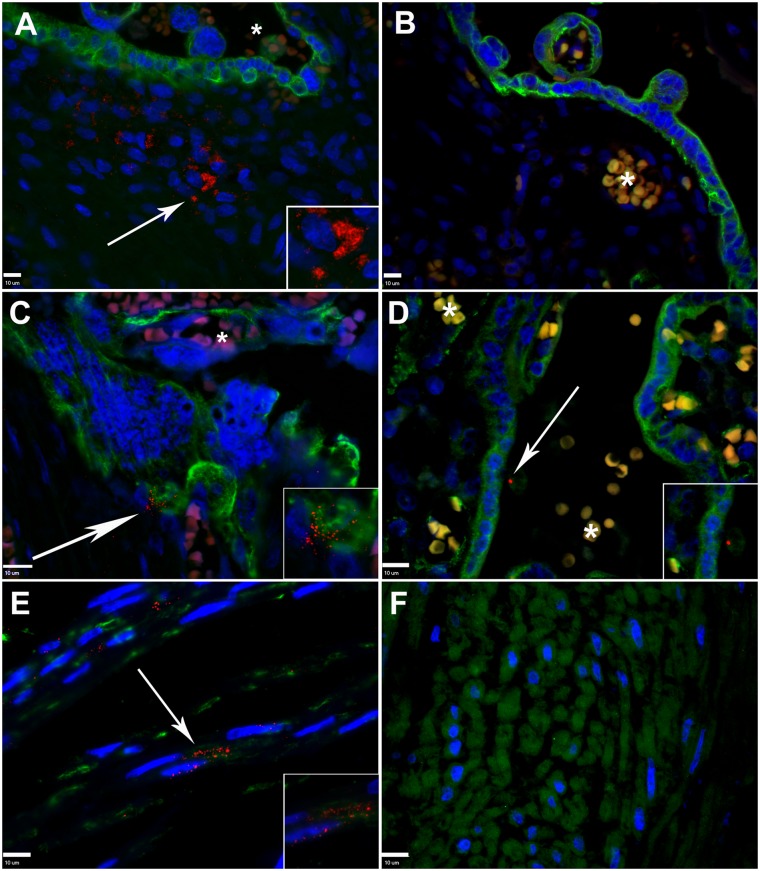
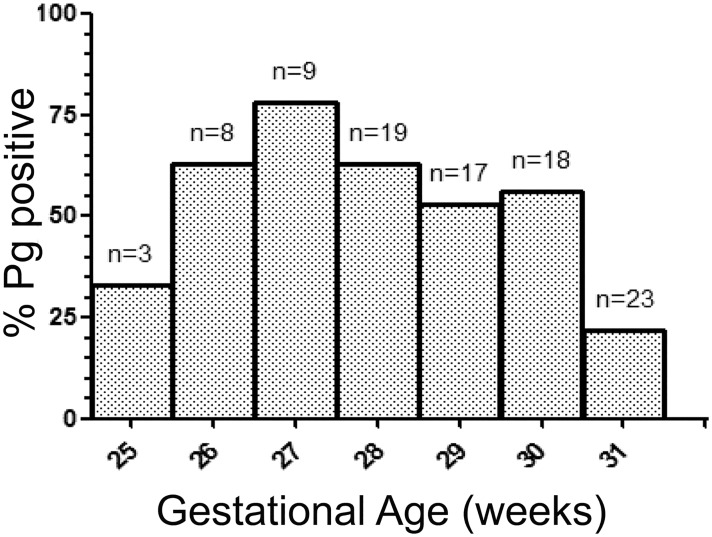
Intrauterine presence of Porphyromonas gingivalis (Pg), a common oral pathobiont, is implicated in preterm birth. Our aim was to determine if the location of Pg within placental and/or umbilical cord sections was associated with a specific delivery diagnosis at preterm delivery (histologic chorioamnionitis, chorioamnionitis with funisitis, preeclampsia, and preeclampsia with HELLP-syndrome, small for gestational age). The prevalence and location of Pg within archived placental and umbilical cord specimens from preterm (25 to 32 weeks gestation) and term control cohorts were evaluated by immunofluorescent histology. Detection of Pg was performed blinded to pregnancy characteristics. Multivariate analyses were performed to evaluate independent effects of gestational age, being small for gestational age, specific preterm delivery diagnosis, antenatal steroids, and delivery mode, on the odds of having Pg in the preterm tissue. Within the preterm cohort, 49 of 97 (51%) placentas and 40 of 97 (41%) umbilical cord specimens were positive for Pg. Pg within the placenta was significantly associated with shorter gestation lengths (OR 0.63 (95%CI: 0.48-0.85; p = 0.002) per week) and delivery via caesarean section (OR 4.02 (95%CI: 1.15-14.04; p = 0.03), but not with histological chorioamnionitis or preeclampsia. However, the presence of Pg in the umbilical cord was significantly associated with preeclampsia: OR 6.73 (95%CI: 1.31-36.67; p = 0.02). In the term cohort, 2 of 35 (6%) placentas and no umbilical cord term specimens were positive for Pg. The location of Pg within the placenta was different between preterm and term groups in that Pg within the villous mesenchyme was only detected in the preterm cohort, whereas Pg associated with syncytiotrophoblasts was found in both preterm and term placentas. Taken together, our results suggest that the presence of Pg within the villous stroma or umbilical cord may be an important determinant in Pg-associated adverse pregnancy outcomes.
牙龈卟啉单胞菌(Pg)作为一种常见的口腔致病共生菌,其在子宫内的存在与早产有关。我们的目的是确定Pg在胎盘和/或脐带切片中的位置是否与早产时的特定分娩诊断相关(组织学绒毛膜羊膜炎、伴有脐带炎的绒毛膜羊膜炎、先兆子痫、伴有HELLP综合征的先兆子痫、小于胎龄)。通过免疫荧光组织学评估来自早产(妊娠25至32周)和足月对照队列的存档胎盘和脐带标本中Pg的患病率和位置。Pg的检测在不了解妊娠特征的情况下进行。进行多变量分析以评估胎龄、小于胎龄、特定的早产分娩诊断、产前类固醇和分娩方式对早产组织中存在Pg几率的独立影响。在早产队列中,97个胎盘中的49个(51%)和97个脐带标本中的40个(41%)Pg呈阳性。胎盘中的Pg与较短的妊娠长度显著相关(每周OR 0.63(95%CI:0.48 - 0.85;p = 0.002))以及剖宫产分娩(OR 4.02(95%CI:1.15 - 14.04;p = 0.03)),但与组织学绒毛膜羊膜炎或先兆子痫无关。然而,脐带中Pg的存在与先兆子痫显著相关:OR 6.73(95%CI:1.31 - 36.67;p = 0.02)。在足月队列中,35个胎盘中的2个(6%)Pg呈阳性,足月脐带标本均未检测到Pg阳性。早产组和足月组胎盘中Pg的位置不同,因为仅在早产队列中检测到绒毛间质内的Pg,而在早产和足月胎盘中均发现与合体滋养层相关的Pg。综上所述,我们的结果表明绒毛基质或脐带中Pg的存在可能是与Pg相关的不良妊娠结局的重要决定因素。