Wang Qianyi, Afshin Ashkan, Yakoob Mohammad Yawar, Singh Gitanjali M, Rehm Colin D, Khatibzadeh Shahab, Micha Renata, Shi Peilin, Mozaffarian Dariush
Harvard T.H. Chan School of Public Health, Boston, MA (Q.W., M.Y.Y., S.K.).
Friedman School of Nutrition Science & Policy, Tufts University, Boston, MA (A.A., G.M.S., C.D.R., R.M., P.S., D.M.).
J Am Heart Assoc. 2016 Jan 20;5(1):e002891. doi: 10.1161/JAHA.115.002891.
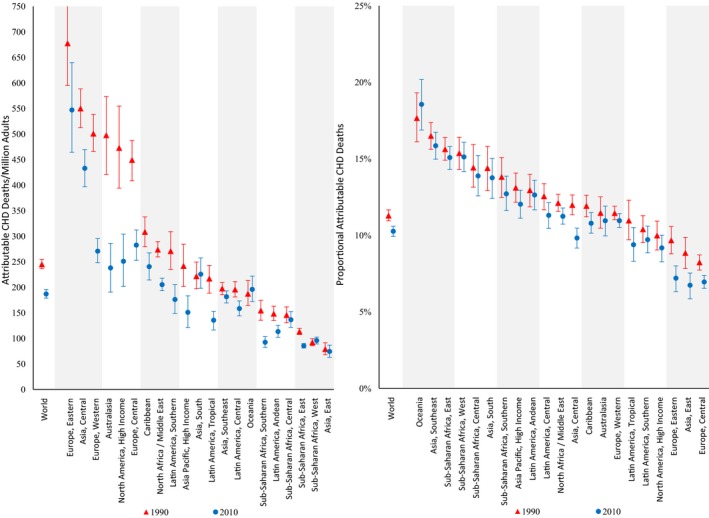
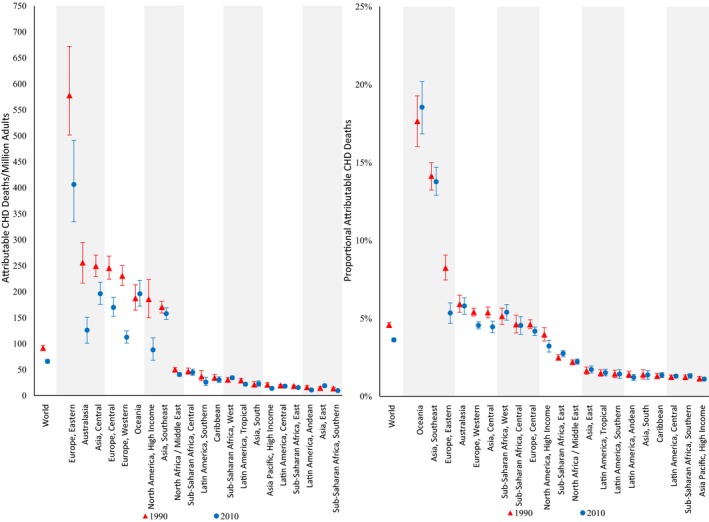
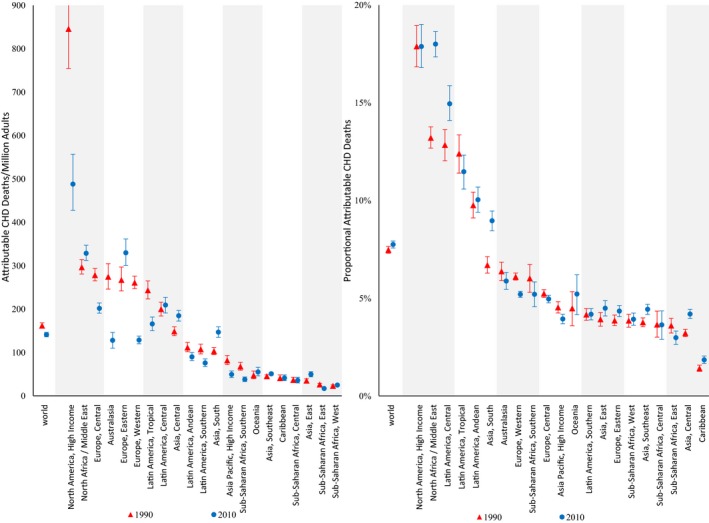
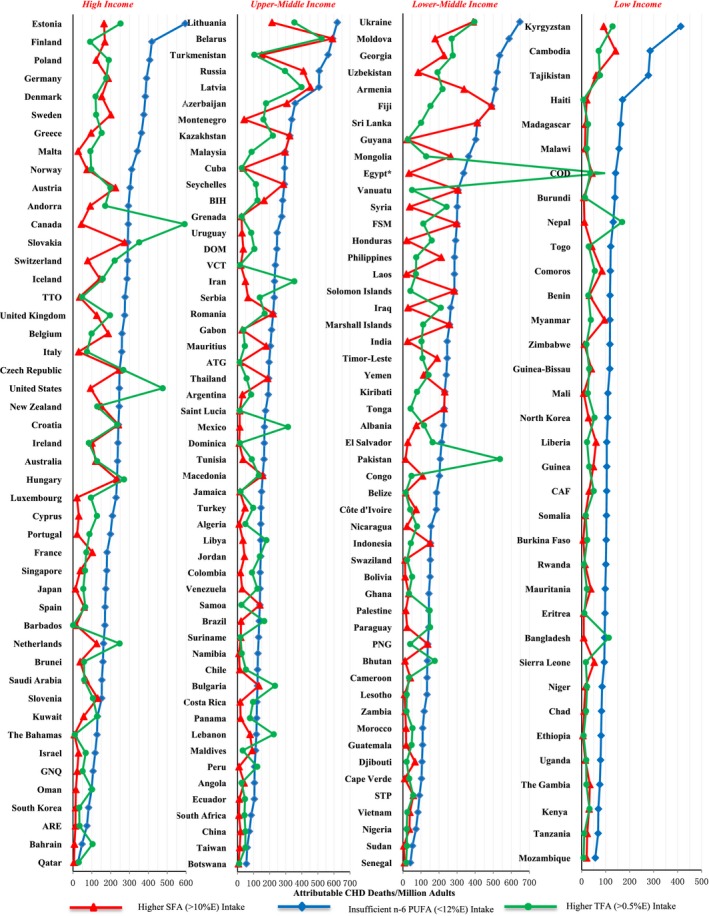
Saturated fat (SFA), ω-6 (n-6) polyunsaturated fat (PUFA), and trans fat (TFA) influence risk of coronary heart disease (CHD), but attributable CHD mortalities by country, age, sex, and time are unclear.
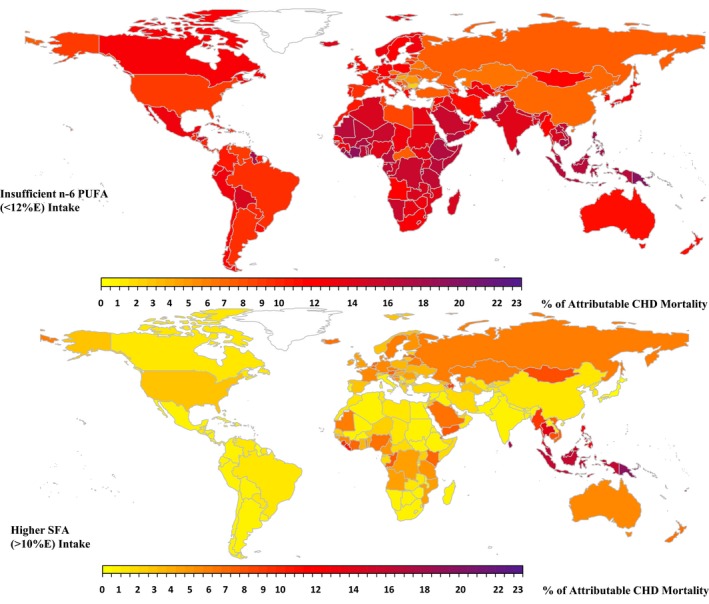
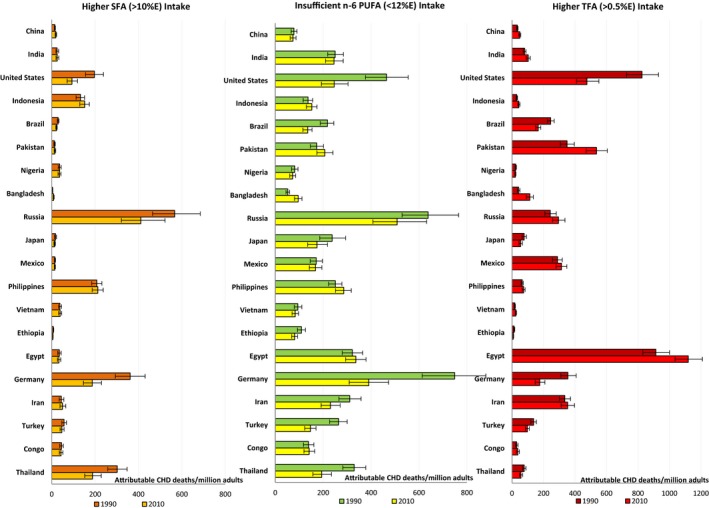
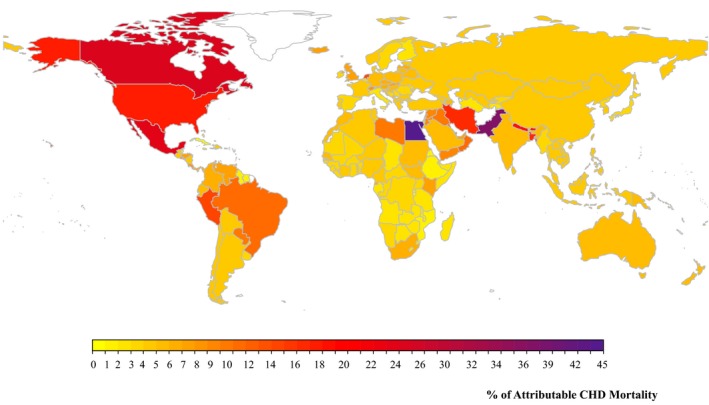
National intakes of SFA, n-6 PUFA, and TFA were estimated using a Bayesian hierarchical model based on country-specific dietary surveys; food availability data; and, for TFA, industry reports on fats/oils and packaged foods. Etiologic effects of dietary fats on CHD mortality were derived from meta-analyses of prospective cohorts and CHD mortality rates from the 2010 Global Burden of Diseases study. Absolute and proportional attributable CHD mortality were computed using a comparative risk assessment framework. In 2010, nonoptimal intakes of n-6 PUFA, SFA, and TFA were estimated to result in 711 800 (95% uncertainty interval [UI] 680 700-745 000), 250 900 (95% UI 236 900-265 800), and 537 200 (95% UI 517 600-557 000) CHD deaths per year worldwide, accounting for 10.3% (95% UI 9.9%-10.6%), 3.6%, (95% UI 3.5%-3.6%) and 7.7% (95% UI 7.6%-7.9%) of global CHD mortality. Tropical oil-consuming countries were estimated to have the highest proportional n-6 PUFA- and SFA-attributable CHD mortality, whereas Egypt, Pakistan, and Canada were estimated to have the highest proportional TFA-attributable CHD mortality. From 1990 to 2010 globally, the estimated proportional CHD mortality decreased by 9% for insufficient n-6 PUFA and by 21% for higher SFA, whereas it increased by 4% for higher TFA, with the latter driven by increases in low- and middle-income countries.
Nonoptimal intakes of n-6 PUFA, TFA, and SFA each contribute to significant estimated CHD mortality, with important heterogeneity across countries that informs nation-specific clinical, public health, and policy priorities.
饱和脂肪(SFA)、ω-6(n-6)多不饱和脂肪(PUFA)和反式脂肪(TFA)会影响冠心病(CHD)风险,但各国、各年龄、各性别以及各时间段中可归因于这些脂肪的冠心病死亡率尚不清楚。
基于特定国家的饮食调查、食物供应数据以及(针对TFA的)油脂和包装食品行业报告,使用贝叶斯分层模型估算各国SFA、n-6 PUFA和TFA的摄入量。膳食脂肪对冠心病死亡率的病因学影响源自前瞻性队列的荟萃分析以及《2010年全球疾病负担研究》中的冠心病死亡率。使用比较风险评估框架计算绝对和比例可归因冠心病死亡率。2010年,据估计,n-6 PUFA、SFA和TFA摄入不当分别导致全球每年711800例(95%不确定区间[UI] 680700 - 745000)、250900例(95% UI 236900 - 265800)和537200例(95% UI 517600 - 557000)冠心病死亡,分别占全球冠心病死亡率的10.3%(95% UI 9.9% - 10.6%)、3.6%(95% UI 3.5% - 3.6%)和7.7%(95% UI 7.6% - 7.9%)。据估计,消费热带油的国家中,n-6 PUFA和SFA归因的冠心病死亡率比例最高,而埃及、巴基斯坦和加拿大的TFA归因冠心病死亡率比例最高。从1990年到2010年全球范围来看,n-6 PUFA摄入不足导致的冠心病死亡率比例估计下降了9%,SFA摄入过多导致的下降了21%,而TFA摄入过多导致的上升了4%,后者主要是由低收入和中等收入国家的增长推动的。
n-6 PUFA、TFA和SFA摄入不当均导致了显著的估计冠心病死亡率,各国之间存在重要的异质性,这为各国特定的临床、公共卫生和政策重点提供了依据。