Wu Lei, He Yao, Jiang Bin, Zuo Fang, Liu Qinghui, Zhang Li, Zhou Changxi, Liu Miao, Chen Hongyan, Cheng K K, Chan Sophia S C, Lam Tai Hing
Department of Epidemiology, Institute of Geriatrics, Chinese PLA General Hospital, 28 Fuxing Road, Beijing, 100853, China.
Beijing Key Laboratory of Aging and Geriatrics, Chinese PLA General Hospital, Institute of Geriatrics, 28 Fuxing Road, Beijing, 100853, China.
BMC Public Health. 2016 Jan 22;16:63. doi: 10.1186/s12889-016-2718-5.
No previous studies have investigated whether additional telephone follow-up counseling sessions after face-to-face counseling can increase quitting in China, and whether this strategy is feasible and effective for promoting smoking cessation is still unclear.
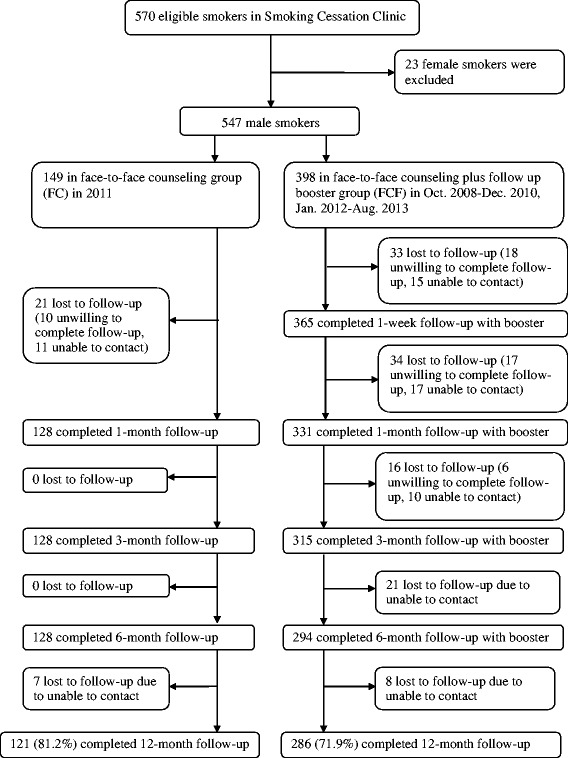
A non-randomized controlled study was conducted in Beijing. We compared the quit rates of one group which received face-to-face counseling (FC) alone (one session of 40 min) to another group which received the same face-to-face counseling plus four follow-up sessions of brief telephone counseling (15-20 min each) at 1 week, 1, 3 and 6 month follow-up (FCF). No smoking cessation medication was provided. From October 2008 to August 2013, Chinese male smokers who sought treatment in a part-time regular smoking cessation clinic of a large general hospital in Beijing were invited to participate in the present study. Eligible male smokers (n = 547) were divided into two groups: FC (n = 149) and FCF (n = 398). Main outcomes were self-reported 7-day point prevalence and 6 month continuous quit rates at 12 month follow-up.
By intention to treat, at 12 month follow-up, the 7-day point prevalence and 6 month continuous quit rates of FC and FCF were 14.8 % and 26.4 %, and 10.7 % and 19.6 % respectively. The adjusted odds ratios (95 % confidence intervals) of quitting in FCF compared to FC was 2.34 (1.34-4.10) (P = 0.003) and 2.41 (1.28-4.52) (P = 0.006), respectively. Stepwise logistic regression showed that FCF, being married, unemployed and a lower Fagerström score were significant independent predictors of 6 month continuous quitting at 12 month follow-up.
Using systematically collected data from real-world practice, our smoking cessation clinic has shown that the additional telephone follow-up counseling sessions doubled the quit rate.
此前尚无研究调查在中国,面对面咨询后增加电话随访咨询是否能提高戒烟成功率,且该策略对促进戒烟是否可行及有效仍不明确。
在北京开展了一项非随机对照研究。我们将仅接受面对面咨询(一次40分钟)的一组与另一组进行比较,后者除接受相同的面对面咨询外,还在1周、1个月、3个月和6个月随访时接受4次简短电话咨询(每次15 - 20分钟)(面对面咨询加电话随访咨询)。未提供戒烟药物。2008年10月至2013年8月,邀请在北京一家大型综合医院兼职的正规戒烟门诊寻求治疗的中国男性吸烟者参与本研究。符合条件的男性吸烟者(n = 547)分为两组:面对面咨询组(n = 149)和面对面咨询加电话随访咨询组(n = 398)。主要结局指标为在12个月随访时自我报告的7天时点患病率和6个月持续戒烟率。
按意向性分析,在12个月随访时,面对面咨询组和面对面咨询加电话随访咨询组的7天时点患病率分别为14.8%和26.4%,6个月持续戒烟率分别为10.7%和19.6%。与面对面咨询组相比,面对面咨询加电话随访咨询组戒烟的调整优势比(95%置信区间)分别为2.34(1.34 - 4.10)(P = 0.003)和2.41(1.28 - 4.52)(P = 0.006)。逐步逻辑回归显示,面对面咨询加电话随访咨询、已婚、失业以及较低的法格斯特龙评分是12个月随访时6个月持续戒烟的显著独立预测因素。
通过来自实际临床实践的系统收集数据,我们的戒烟门诊表明,额外的电话随访咨询使戒烟率提高了一倍。