UWI Solutions for Developing Countries, University of the West Indies, Mona, Kingston, Jamaica.
Liggins Institute and National Research Centre for Growth and Development, University of Auckland, Auckland, New Zealand Charles Perkins Centre and School of Biological Sciences, The University of Sydney, Sydney, NSW, Australia Faculty of Veterinary Sciences, The University of Sydney, Sydney, NSW, Australia.
Evol Med Public Health. 2016 May 18;2016(1):158-69. doi: 10.1093/emph/eov030. Print 2016.
Birthweight differences between kwashiorkor and marasmus suggest that intrauterine factors influence the development of these syndromes of malnutrition and may modulate risk of obesity through dietary intake. We tested the hypotheses that the target protein intake in adulthood is associated with birthweight, and that protein leveraging to maintain this target protein intake would influence energy intake (EI) and body weight in adult survivors of malnutrition.
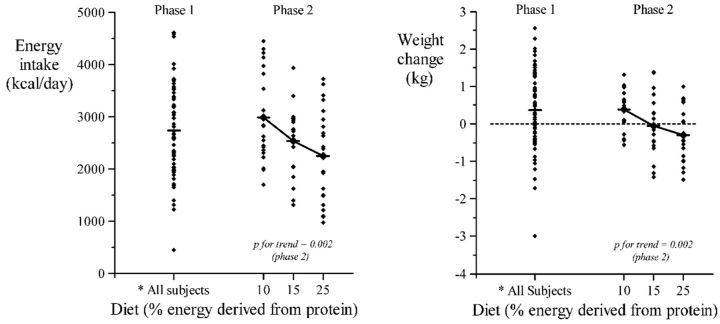
Sixty-three adult survivors of marasmus and kwashiorkor could freely compose a diet from foods containing 10, 15 and 25 percentage energy from protein (percentage of energy derived from protein (PEP); Phase 1) for 3 days. Participants were then randomized in Phase 2 (5 days) to diets with PEP fixed at 10%, 15% or 25%.
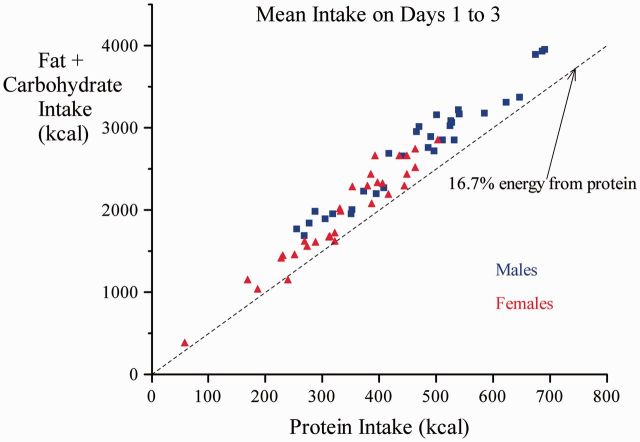
Self-selected PEP was similar in both groups. In the groups combined, selected PEP was 14.7, which differed significantly (P < 0.0001) from the null expectation (16.7%) of no selection. Self-selected PEP was inversely related to birthweight, the effect disappearing after adjusting for sex and current body weight. In Phase 2, PEP correlated inversely with EI (P = 0.002) and weight change from Phase 1 to 2 (P = 0.002). Protein intake increased with increasing PEP, but to a lesser extent than energy increased with decreasing PEP.
Macronutrient intakes were not independently related to birthweight or diagnosis. In a free-choice situation (Phase 1), subjects selected a dietary PEP significantly lower than random. Lower PEP diets induce increased energy and decreased protein intake, and are associated with weight gain.
消瘦症和夸希奥科病患儿的出生体重存在差异,这表明宫内因素会影响这些营养不良综合征的发生发展,并可能通过饮食摄入来调节肥胖风险。本研究旨在检验以下两个假设:一是成年人的目标蛋白质摄入量与出生体重相关;二是为维持目标蛋白质摄入量而进行的蛋白质补充会影响营养不良成年幸存者的能量摄入(EI)和体重。
63 名消瘦症和夸希奥科病成年幸存者可从含有 10%、15%和 25%能量蛋白质的食物中自由搭配饮食(蛋白质能量比(PEP);第 1 阶段),持续 3 天。然后,参与者在第 2 阶段(5 天)随机分为 PEP 固定为 10%、15%或 25%的饮食组。
两组的自我选择 PEP 相似。在合并组中,选择的 PEP 为 14.7%,与无选择的预期值(16.7%)差异显著(P < 0.0001)。自我选择的 PEP 与出生体重呈负相关,调整性别和当前体重后,这种相关性消失。在第 2 阶段,PEP 与 EI 呈负相关(P = 0.002),与第 1 阶段到第 2 阶段的体重变化呈负相关(P = 0.002)。PEP 增加与蛋白质摄入量增加相关,但与能量摄入量减少相比,蛋白质摄入量增加的程度较小。
宏量营养素摄入量与出生体重或诊断无独立关系。在自由选择的情况下(第 1 阶段),受试者选择的饮食 PEP 明显低于随机选择。低 PEP 饮食会增加能量和减少蛋白质摄入,并与体重增加相关。