Fink Ericka L, Berger Rachel P, Clark Robert S B, Watson R Scott, Angus Derek C, Panigrahy Ashok, Richichi Rudolph, Callaway Clifton W, Bell Michael J, Mondello Stefania, Hayes Ronald L, Kochanek Patrick M
Critical Care Medicine, Children's Hospital of Pittsburgh of UPMC, Pittsburgh, PA, USA; Clinical Research, Investigation, and Systems Modeling of Acute Illness (CRISMA) Center, Pittsburgh, PA, USA; Safar Center for Resuscitation Research, Pittsburgh, PA, USA.
Child Advocacy, Pediatrics, Children's Hospital of Pittsburgh of UPMC, Pittsburgh, PA, USA.
Resuscitation. 2016 Apr;101:65-70. doi: 10.1016/j.resuscitation.2016.01.024. Epub 2016 Feb 6.
Brain injury is the leading cause of morbidity and death following pediatric cardiac arrest. Serum biomarkers of brain injury may assist in outcome prognostication. The objectives of this study were to evaluate the properties of serum ubiquitin carboxyl-terminal esterase-L1 (UCH-L1) and glial fibrillary acidic protein (GFAP) to classify outcome in pediatric cardiac arrest.
Single center prospective study. Serum biomarkers were measured at 2 time points during the initial 72 h in children after cardiac arrest (n=19) and once in healthy children (controls, n=43). We recorded demographics and details of the cardiac arrest and resuscitation. We determined the associations between serum biomarker concentrations and Pediatric Cerebral Performance Category (PCPC) at 6 months (favorable (PCPC 1-3) or unfavorable (PCPC 4-6)).
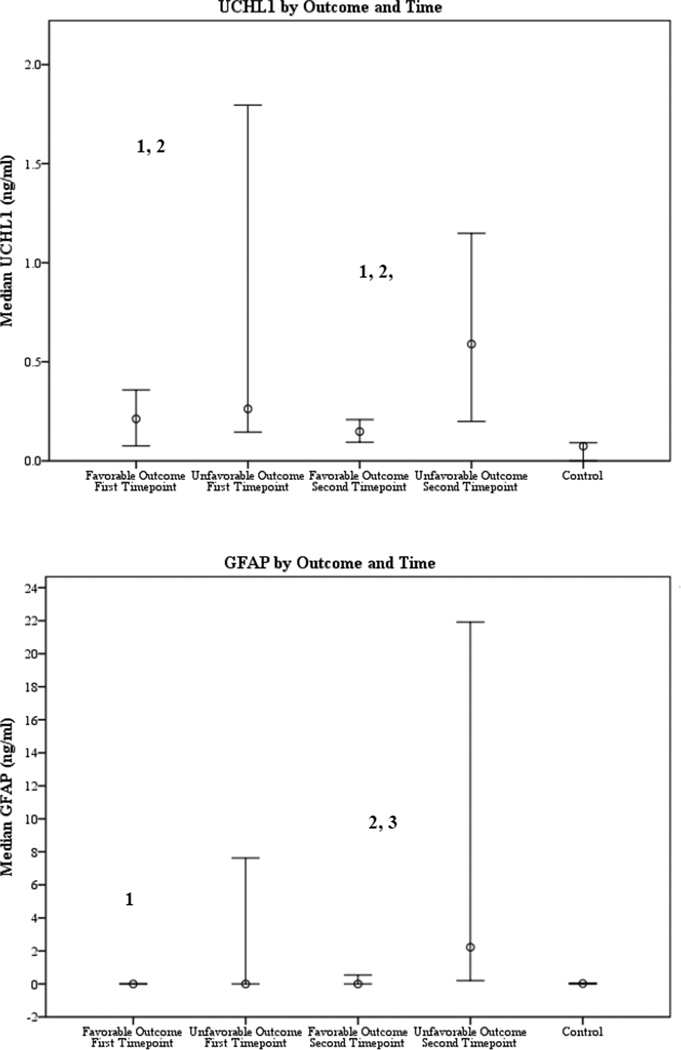
The initial assessment (time point 1) occurred at a median (IQR) of 10.5 (5.5-17.0)h and the second assessment (time point 2) at 59.0 (54.5-65.0)h post-cardiac arrest. Serum UCH-L1 was higher among children following cardiac arrest than among controls at both time points (p<0.05). Serum GFAP in subjects with unfavorable outcome was higher at time point 2 than in controls (p<0.05). Serum UCH-L1 at time point 1 (AUC 0.782) and both UCH-L1 and GFAP at time point 2 had good classification accuracy for outcome (AUC 0.822 and 0.796), p<0.05 for all.
Preliminary data suggest that serum UCH-L1 and GFAP may be of use to prognosticate outcome after pediatric cardiac arrest at clinically-relevant time points and should be validated prospectively.
脑损伤是小儿心脏骤停后发病和死亡的主要原因。脑损伤的血清生物标志物可能有助于预后评估。本研究的目的是评估血清泛素羧基末端水解酶-L1(UCH-L1)和胶质纤维酸性蛋白(GFAP)对小儿心脏骤停预后进行分类的特性。
单中心前瞻性研究。在心脏骤停后的儿童(n=19)初始72小时内的2个时间点测量血清生物标志物,在健康儿童(对照组,n=43)中测量一次。我们记录了人口统计学资料以及心脏骤停和复苏的详细情况。我们确定了血清生物标志物浓度与6个月时小儿脑功能表现分类(PCPC)之间的关联(良好(PCPC 1-3)或不良(PCPC 4-6))。
首次评估(时间点1)发生在心脏骤停后中位数(IQR)为10.5(5.5-17.0)小时,第二次评估(时间点2)发生在59.0(54.5-65.0)小时。在两个时间点,心脏骤停后的儿童血清UCH-L1均高于对照组(p<0.05)。预后不良的受试者在时间点2的血清GFAP高于对照组(p<0.05)。时间点1的血清UCH-L1(AUC 0.782)以及时间点2的UCH-L1和GFAP对预后均具有良好的分类准确性(AUC 0.822和0.796),所有p均<0.05。
初步数据表明,血清UCH-L1和GFAP可能有助于在临床相关时间点预测小儿心脏骤停后的预后,应进行前瞻性验证。