Pinault Lauren, Tjepkema Michael, Crouse Daniel L, Weichenthal Scott, van Donkelaar Aaron, Martin Randall V, Brauer Michael, Chen Hong, Burnett Richard T
Health Analysis Division, Statistics Canada, 100 Tunney's Pasture Driveway, Ottawa, ON, K1A 0T6, Canada.
New Brunswick Institute for Research, Data, and Training (NB-IRDT) and Department of Sociology, University of New Brunswick, Fredericton, NB, PO Box 4400, E3B 5A3, Canada.
Environ Health. 2016 Feb 11;15:18. doi: 10.1186/s12940-016-0111-6.
Understanding the shape of the relationship between long-term exposure to ambient fine particulate matter (PM2.5) concentrations and health risks is critical for health impact and risk assessment. Studies evaluating the health risks of exposure to low concentrations of PM2.5 are limited. Further, many existing studies lack individual-level information on potentially important behavioural confounding factors.
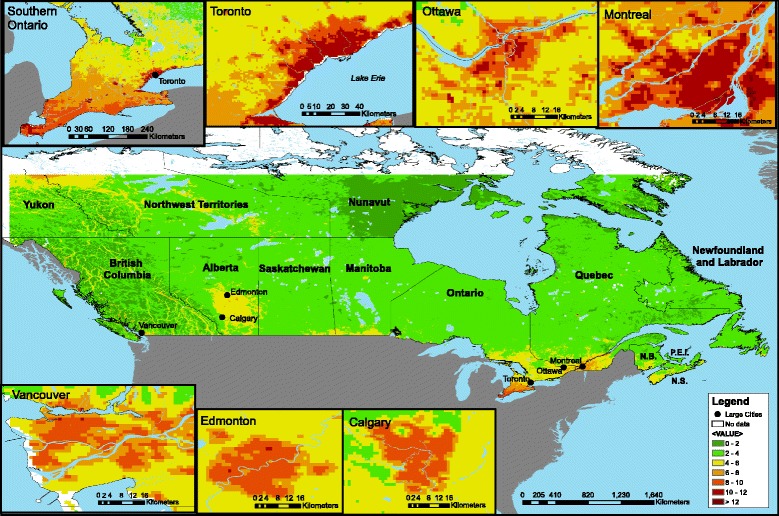
A prospective cohort study was conducted among a subset of participants in a cohort that linked respondents of the Canadian Community Health Survey to mortality (n = 299,500) with satellite-derived ambient PM2.5 estimates. Participants enrolled between 2000 and 2008 were followed to date of death or December 31, 2011. Cox proportional hazards models were used to estimate hazard ratios (HRs) for mortality attributed to PM2.5 exposure, adjusted for individual-level and contextual covariates, including smoking behaviour and body mass index (BMI).
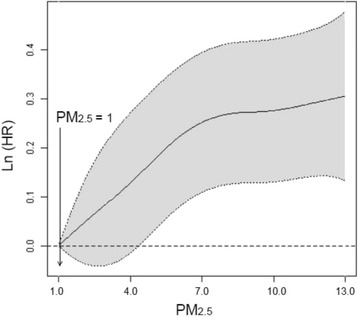
Approximately 26,300 non-accidental deaths, of which 32.5 % were due to circulatory disease and 9.1 % were due to respiratory disease, occurred during the follow-up period. Ambient PM2.5 exposures were relatively low (mean = 6.3 μg/m(3)), yet each 10 μg/m(3) increase in exposure was associated with increased risks of non-accidental (HR = 1.26; 95 % CI: 1.19-1.34), circulatory disease (HR = 1.19; 95 % CI: 1.07-1.31), and respiratory disease mortality (HR = 1.52; 95 % CI: 1.26-1.84) in fully adjusted models. Higher hazard ratios were observed for respiratory mortality among respondents who never smoked (HR = 1.97; 95 % CI: 1.24-3.13 vs. HR = 1.45; 95 % CI: 1.17-1.79 for ever smokers), and among obese (BMI ≥ 30) respondents (HR = 1.76; 95 % CI: 1.15-2.69 vs. HR = 1.41; 95 % CI: 1.04-1.91 for normal weight respondents), though differences between groups were not statistically significant. A threshold analysis for non-accidental mortality estimated a threshold concentration of 0 μg/m(3) (+95 % CI = 4.5 μg/m(3)).
Increased risks of non-accidental, circulatory, and respiratory mortality were observed even at very low concentrations of ambient PM2.5. HRs were generally greater than most literature values, and adjusting for behavioural covariates served to reduce HR estimates slightly.
了解长期暴露于环境细颗粒物(PM2.5)浓度与健康风险之间的关系形态对于健康影响和风险评估至关重要。评估低浓度PM2.5暴露健康风险的研究有限。此外,许多现有研究缺乏关于潜在重要行为混杂因素的个体层面信息。
在一个队列的部分参与者中进行了一项前瞻性队列研究,该队列将加拿大社区健康调查的受访者与卫星衍生的环境PM2.5估计值与死亡率(n = 299,500)相联系。对2000年至2008年期间入组的参与者随访至死亡日期或2011年12月31日。使用Cox比例风险模型估计归因于PM2.5暴露的死亡率的风险比(HRs),并针对个体层面和背景协变量进行调整,包括吸烟行为和体重指数(BMI)。
在随访期间发生了约26,300例非意外死亡,其中32.5% 归因于循环系统疾病,9.1% 归因于呼吸系统疾病。环境PM2.5暴露相对较低(平均值 = 6.3 μg/m³),但在完全调整的模型中,每增加10 μg/m³ 的暴露与非意外死亡(HR = 1.26;95% CI:1.19 - 1.34)、循环系统疾病(HR = 1.19;95% CI:1.07 - 1.31)和呼吸系统疾病死亡率(HR = 1.52;95% CI:1.26 - 1.84)风险增加相关。在从不吸烟的受访者中观察到呼吸系统死亡率的风险比更高(HR = 1.97;95% CI:1.24 - 3.13,而曾经吸烟者的HR = 1.45;95% CI:1.17 - 1.79),在肥胖(BMI≥30)受访者中也是如此(HR = 1.76;95% CI:1.15 - 2.69,而正常体重受访者的HR = 1.41;9% CI:1.04 - 1.91),尽管组间差异无统计学意义。非意外死亡率的阈值分析估计阈值浓度为0 μg/m³(+95% CI = 4.5 μg/m³)。
即使在环境PM2.5浓度非常低的情况下,也观察到非意外、循环系统和呼吸系统死亡率风险增加。风险比通常高于大多数文献值,并且针对行为协变量进行调整可使风险比估计值略有降低。