Win Aye A, Imwong Mallika, Kyaw Myat P, Woodrow Charles J, Chotivanich Kesinee, Hanboonkunupakarn Borimas, Pukrittayakamee Sasithon
Department of Medicine, Institute of Medicine 1, Yangon, Myanmar.
Department of Molecular Tropical Medicine and Genetics, Mahidol University, Bangkok, Thailand.
Malar J. 2016 Feb 24;15:110. doi: 10.1186/s12936-016-1147-3.
Artemisinin-based combination therapy has been first-line treatment for falciparum malaria in Myanmar since 2005. The wide extent of artemisinin resistance in the Greater Mekong sub-region and the presence of mefloquine resistance at the Myanmar-Thailand border raise concerns over resistance patterns in Myanmar. The availability of molecular markers for resistance to both drugs enables assessment even in remote malaria-endemic areas.
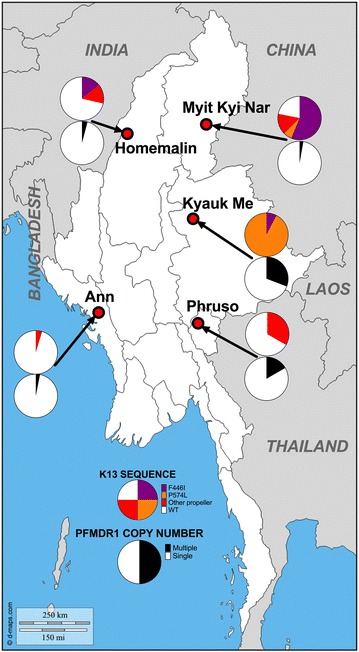
A total of 250 dried blood spot samples collected from patients with Plasmodium falciparum malarial infection in five malaria-endemic areas across Myanmar were analysed for kelch 13 sequence (k13) and pfmdr1 copy number variation. K13 mutations in the region corresponding to amino acids 210-726 (including the propeller region of the protein) were detected by nested PCR amplification and sequencing, and pfmdr1 copy number variation by real-time PCR. In two sites, a sub-set of patients were prospectively followed up for assessment of day-3 parasite clearance rates after a standard course of artemether-lumefantrine.
K13 mutations and pfmdr1 amplification were successfully analysed in 206 and 218 samples, respectively. Sixty-nine isolates (33.5 %) had mutations within the k13 propeller region with 53 of these (76.8 %) having mutations already known to be associated with artemisinin resistance. F446I (32 isolates) and P574L (15 isolates) were the most common examples. K13 mutation was less common in sites in western border regions (29 of 155 isolates) compared to samples from the east and north (40 of 51 isolates; p < 0.0001). The overall proportion of parasites with multiple pfmdr1 copies (greater than 1.5) was 5.5 %. Seven samples showed both k13 mutation and multiple copies of pfmdr1. Only one of 36 patients followed up after artemether-lumefantrine treatment still had parasites at day 3; molecular analysis indicated wild-type k13 and single copy pfmdr1.
The proportion of P. falciparum isolates with mutations in the propeller region of k13 indicates that artemisinin resistance extends across much of Myanmar. There is a low prevalence of parasites with multiple pfmdr1 copies across the country. The efficacy of artemisinin-based combination therapy containing mefloquine and lumefantrine is, therefore, expected to be high, although regular monitoring of efficacy will be important.
自2005年以来,以青蒿素为基础的联合疗法一直是缅甸恶性疟的一线治疗方法。大湄公河次区域青蒿素耐药性广泛存在,且缅甸与泰国边境存在甲氟喹耐药性,这引发了对缅甸耐药模式的担忧。两种药物耐药性分子标记的可用性使得即使在偏远的疟疾流行地区也能进行评估。
对从缅甸五个疟疾流行地区的恶性疟感染患者收集的250份干血斑样本进行分析,检测kelch 13序列(k13)和pfmdr1拷贝数变异。通过巢式PCR扩增和测序检测对应于氨基酸210 - 726区域(包括该蛋白的螺旋桨区域)的k13突变,通过实时PCR检测pfmdr1拷贝数变异。在两个地点,对一部分患者进行前瞻性随访,以评估蒿甲醚 - 本芴醇标准疗程后第3天的寄生虫清除率。
分别成功分析了206份和218份样本中的k13突变和pfmdr1扩增情况。69株分离株(33.5%)在k13螺旋桨区域存在突变,其中53株(76.8%)具有已知与青蒿素耐药性相关的突变。F446I(32株)和P574L(15株)是最常见的例子。与东部和北部的样本相比,西部边境地区的位点k13突变较少见(155株分离株中有29株,51株分离株中有40株;p < 0.0001)。具有多个pfmdr1拷贝(大于1.5)的寄生虫总体比例为5.5%。7个样本同时显示k13突变和多个pfmdr1拷贝。蒿甲醚 - 本芴醇治疗后随访的36例患者中,只有1例在第3天仍有寄生虫;分子分析表明为野生型k13和单拷贝pfmdr1。
k13螺旋桨区域发生突变的恶性疟分离株比例表明,青蒿素耐药性在缅甸大部分地区都存在。全国范围内具有多个pfmdr1拷贝的寄生虫患病率较低。因此,含甲氟喹和本芴醇的以青蒿素为基础的联合疗法疗效预计较高,尽管定期监测疗效很重要。