Adachi Yayoi, Ishiguro Junko, Kotani Haruru, Hisada Tomoka, Ichikawa Mari, Gondo Naomi, Yoshimura Akiyo, Kondo Naoto, Hattori Masaya, Sawaki Masataka, Fujita Takashi, Kikumori Toyone, Yatabe Yasushi, Kodera Yasuhiro, Iwata Hiroji
Department of Breast Oncology, Aichi Cancer Center Hospital, 1-1, Kanokoden, Chikusaku, Nagoya, 464-8681, Japan.
Department of Transplantation and Endocrine Surgery, Nagoya University Graduate School of Medicine, 65 Tsurumai, Showaku, Nagoya, 466-8560, Japan.
BMC Cancer. 2016 Mar 25;16:248. doi: 10.1186/s12885-016-2275-4.
The pathological and clinical features of invasive lobular carcinoma (ILC) differ from those of invasive ductal carcinoma (IDC). Several studies have indicated that patients with ILC have a better prognosis than those with ductal carcinoma. However, no previous study has considered the molecular subtypes and histological subtypes of ILC. We compared prognosis between IDC and classical, luminal type ILC and developed prognostic factors for early breast cancer patients with classical luminal ILC.
Four thousand one hundred ten breast cancer patients were treated at the Aichi Cancer Center Hospital from 2003 to 2012. We identified 1,661 cases with luminal IDC and 105 cases with luminal classical ILC. We examined baseline characteristics, clinical outcomes, and prognostic factors of luminal ILC.
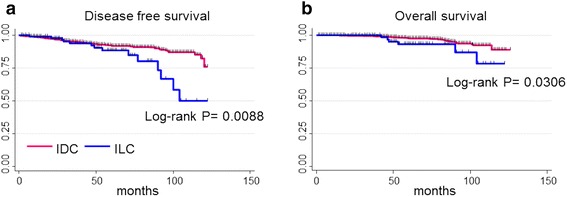
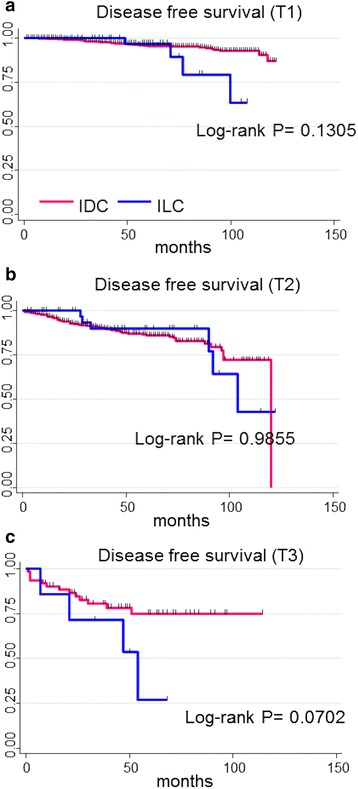
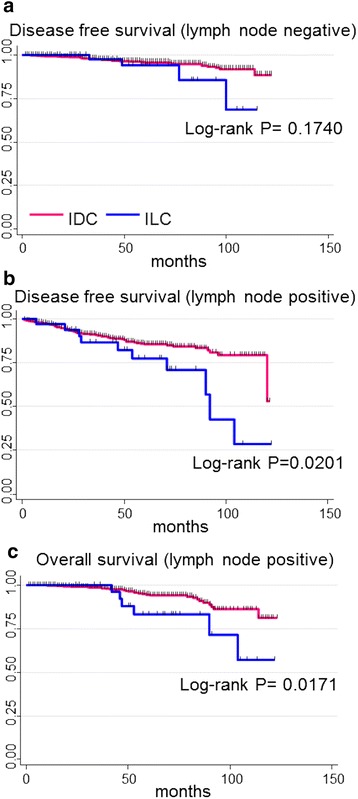
The prognosis of luminal ILC was significantly worse than that of luminal IDC. The rates of 5-year disease free survival (DFS) were 91.9% and 88.4% for patients with luminal IDC and luminal ILC, respectively (P = 0.008). The rates of 5-year overall survival (OS) were 97.6% and 93.1% for patients with luminal IDC and luminal ILC respectively (P = 0.030). Although we analyzed prognosis according to stratification by tumor size, luminal ILC tended to have worse DFS than luminal IDC in the large tumor group. In addition, although our analysis was performed according to matching lymph node status, luminal ILC had a significantly worse DFS and OS than luminal IDC in node-positive patients. Survival curves showed that the prognosis for ILC became worse than IDC over time. Multivariate analysis showed that ILC was an important factor related to higher risk of recurrence of luminal type breast cancer, even when tumor size, lymph node status and histological grade were considered.
Luminal ILC had worse outcomes than luminal IDC. Consequently, different treatment approaches should be used for luminal ILC than for luminal IDC.
浸润性小叶癌(ILC)的病理和临床特征与浸润性导管癌(IDC)不同。多项研究表明,ILC患者的预后优于导管癌患者。然而,此前尚无研究考虑过ILC的分子亚型和组织学亚型。我们比较了IDC与经典腔面型ILC的预后,并为早期经典腔面型ILC乳腺癌患者制定了预后因素。
2003年至2012年期间,爱知县癌症中心医院共治疗了4110例乳腺癌患者。我们确定了1661例腔面型IDC病例和105例腔面型经典ILC病例。我们检查了腔面型ILC的基线特征、临床结局和预后因素。
腔面型ILC的预后明显比腔面型IDC差。腔面型IDC和腔面型ILC患者的5年无病生存率(DFS)分别为91.9%和88.4%(P = 0.008)。腔面型IDC和腔面型ILC患者的5年总生存率(OS)分别为97.6%和93.1%(P = 0.030)。尽管我们根据肿瘤大小分层分析了预后,但在大肿瘤组中,腔面型ILC的DFS往往比腔面型IDC差。此外,尽管我们根据匹配的淋巴结状态进行了分析,但在淋巴结阳性患者中,腔面型ILC的DFS和OS明显比腔面型IDC差。生存曲线显示,随着时间的推移,ILC的预后比IDC更差。多因素分析表明,即使考虑肿瘤大小、淋巴结状态和组织学分级,ILC仍是与腔面型乳腺癌复发风险较高相关的重要因素。
腔面型ILC的结局比腔面型IDC差。因此,对于腔面型ILC应采用与腔面型IDC不同的治疗方法。