Terry Kathryn L, Schock Helena, Fortner Renée T, Hüsing Anika, Fichorova Raina N, Yamamoto Hidemi S, Vitonis Allison F, Johnson Theron, Overvad Kim, Tjønneland Anne, Boutron-Ruault Marie-Christine, Mesrine Sylvie, Severi Gianluca, Dossus Laure, Rinaldi Sabina, Boeing Heiner, Benetou Vassiliki, Lagiou Pagona, Trichopoulou Antonia, Krogh Vittorio, Kuhn Elisabetta, Panico Salvatore, Bueno-de-Mesquita H Bas, Onland-Moret N Charlotte, Peeters Petra H, Gram Inger Torhild, Weiderpass Elisabete, Duell Eric J, Sanchez Maria-Jose, Ardanaz Eva, Etxezarreta Nerea, Navarro Carmen, Idahl Annika, Lundin Eva, Jirström Karin, Manjer Jonas, Wareham Nicholas J, Khaw Kay-Tee, Byrne Karl Smith, Travis Ruth C, Gunter Marc J, Merritt Melissa A, Riboli Elio, Cramer Daniel W, Kaaks Rudolf
Ob/Gyn Epidemiology Center, Brigham and Women's Hospital, Boston, Massachusetts. Obstetrics, Gynecology and Reproductive Biology, Harvard Medical School, Boston, Massachusetts.
Division of Cancer Epidemiology, German Cancer Research Center (DKFZ), Heidelberg, Germany.
Clin Cancer Res. 2016 Sep 15;22(18):4664-75. doi: 10.1158/1078-0432.CCR-16-0316. Epub 2016 Apr 8.
About 60% of ovarian cancers are diagnosed at late stage, when 5-year survival is less than 30% in contrast to 90% for local disease. This has prompted search for early detection biomarkers. For initial testing, specimens taken months or years before ovarian cancer diagnosis are the best source of information to evaluate early detection biomarkers. Here we evaluate the most promising ovarian cancer screening biomarkers in prospectively collected samples from the European Prospective Investigation into Cancer and Nutrition study.
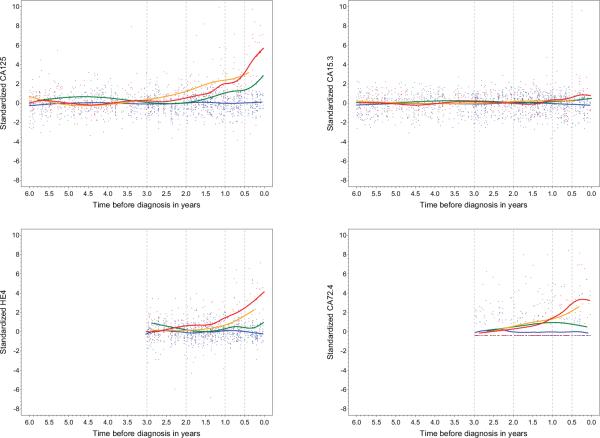
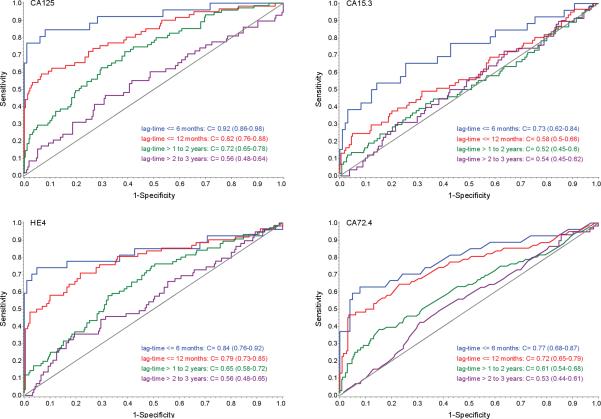
We measured CA125, HE4, CA72.4, and CA15.3 in 810 invasive epithelial ovarian cancer cases and 1,939 controls. We calculated the sensitivity at 95% and 98% specificity as well as area under the receiver operator curve (C-statistic) for each marker individually and in combination. In addition, we evaluated marker performance by stage at diagnosis and time between blood draw and diagnosis.
We observed the best discrimination between cases and controls within 6 months of diagnosis for CA125 (C-statistic = 0.92), then HE4 (0.84), CA72.4 (0.77), and CA15.3 (0.73). Marker performance declined with longer time between blood draw and diagnosis and for earlier staged disease. However, assessment of discriminatory ability at early stage was limited by small numbers. Combinations of markers performed modestly, but significantly better than any single marker.
CA125 remains the single best marker for the early detection of invasive epithelial ovarian cancer, but can be slightly improved by combining with other markers. Identifying novel markers for ovarian cancer will require studies including larger numbers of early-stage cases. Clin Cancer Res; 22(18); 4664-75. ©2016 AACRSee related commentary by Skates, p. 4542.
约60%的卵巢癌在晚期被诊断出来,此时5年生存率低于30%,而局部疾病的5年生存率为90%。这促使人们寻找早期检测生物标志物。对于初始检测,在卵巢癌诊断前数月或数年采集的样本是评估早期检测生物标志物的最佳信息来源。在此,我们在欧洲癌症与营养前瞻性调查研究中前瞻性收集的样本中评估了最有前景的卵巢癌筛查生物标志物。
我们在810例浸润性上皮性卵巢癌病例和1939例对照中测量了CA125、HE4、CA72.4和CA15.3。我们分别计算了每个标志物单独及联合使用时在95%和98%特异性下的敏感性以及受试者操作特征曲线下面积(C统计量)。此外,我们根据诊断时的分期以及采血与诊断之间的时间评估了标志物的性能。
我们观察到,在诊断后6个月内,CA125对病例和对照的区分能力最佳(C统计量 = 0.92),其次是HE4(0.84)、CA72.4(0.77)和CA15.3(0.73)。标志物性能随着采血与诊断之间时间的延长以及疾病分期的提前而下降。然而,早期阶段的鉴别能力评估因病例数量少而受到限制。标志物组合的表现一般,但明显优于任何单个标志物。
CA125仍然是浸润性上皮性卵巢癌早期检测的最佳单一标志物,但与其他标志物联合使用可略有改善。识别卵巢癌的新标志物需要纳入更多早期病例的研究。《临床癌症研究》;22(18);4664 - 75。©2016美国癌症研究协会。见Skates的相关评论,第4542页。