Moteabbed Maryam, Yock Torunn I, Depauw Nicolas, Madden Thomas M, Kooy Hanne M, Paganetti Harald
Radiation Oncology Department, Massachusetts General Hospital and Harvard Medical School, Boston, Massachusetts.
Radiation Oncology Department, Massachusetts General Hospital and Harvard Medical School, Boston, Massachusetts.
Int J Radiat Oncol Biol Phys. 2016 May 1;95(1):190-198. doi: 10.1016/j.ijrobp.2015.12.368. Epub 2015 Dec 29.
This study aimed to assess the clinical impact of spot size and the addition of apertures and range compensators on the treatment quality of pencil beam scanning (PBS) proton therapy and to define when PBS could improve on passive scattering proton therapy (PSPT).
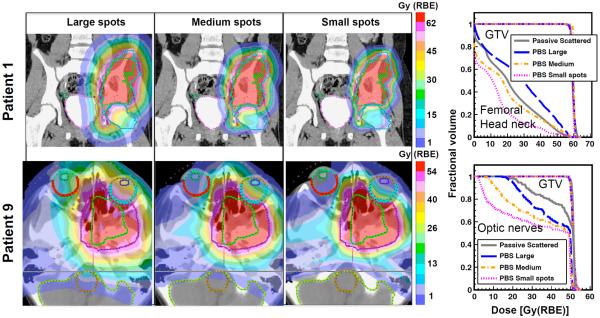
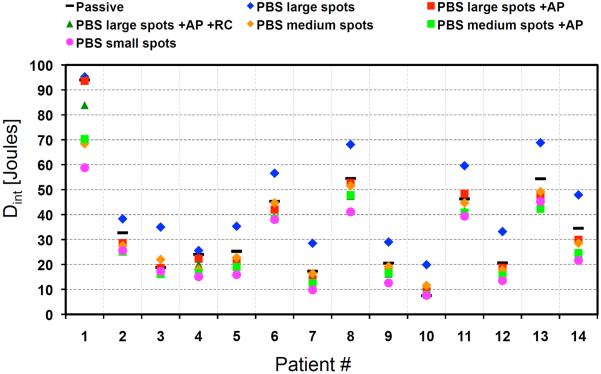
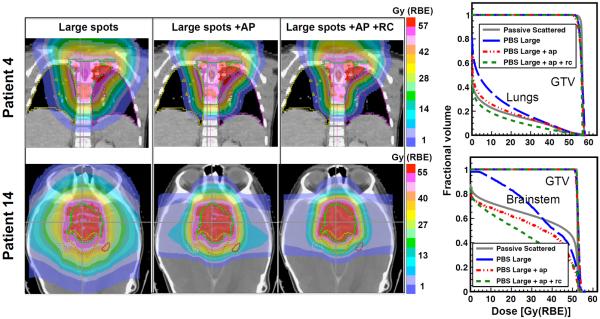
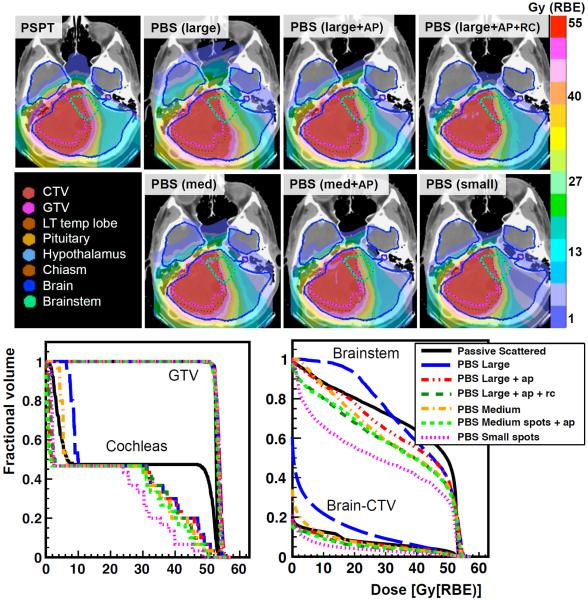
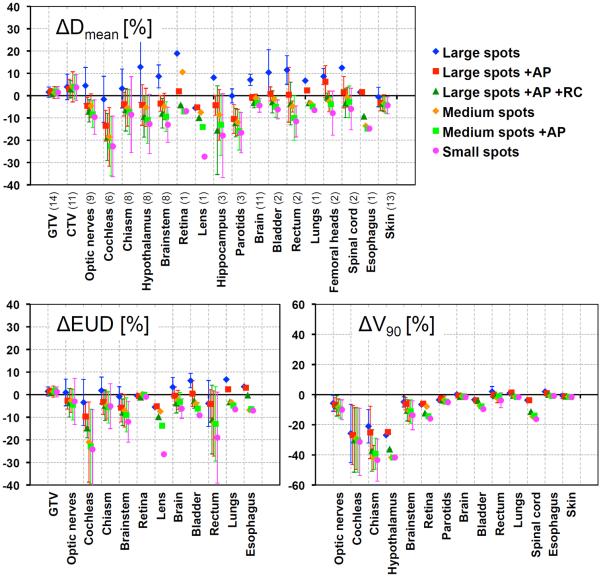
The patient cohort included 14 pediatric patients treated with PSPT. Six PBS plans were created and optimized for each patient using 3 spot sizes (∼12-, 5.4-, and 2.5-mm median sigma at isocenter for 90- to 230-MeV range) and adding apertures and compensators to plans with the 2 larger spots. Conformity and homogeneity indices, dose-volume histogram parameters, equivalent uniform dose (EUD), normal tissue complication probability (NTCP), and integral dose were quantified and compared with the respective PSPT plans.
The results clearly indicated that PBS with the largest spots does not necessarily offer a dosimetric or clinical advantage over PSPT. With comparable target coverage, the mean dose (Dmean) to healthy organs was on average 6.3% larger than PSPT when using this spot size. However, adding apertures to plans with large spots improved the treatment quality by decreasing the average Dmean and EUD by up to 8.6% and 3.2% of the prescribed dose, respectively. Decreasing the spot size further improved all plans, lowering the average Dmean and EUD by up to 11.6% and 10.9% compared with PSPT, respectively, and eliminated the need for beam-shaping devices. The NTCP decreased with spot size and addition of apertures, with maximum reduction of 5.4% relative to PSPT.
The added benefit of using PBS strongly depends on the delivery configurations. Facilities limited to large spot sizes (>∼8 mm median sigma at isocenter) are recommended to use apertures to reduce treatment-related toxicities, at least for complex and/or small tumors.
本研究旨在评估光斑尺寸以及添加准直器和射程补偿器对笔形束扫描(PBS)质子治疗质量的临床影响,并确定PBS何时能优于被动散射质子治疗(PSPT)。
患者队列包括14例接受PSPT治疗的儿科患者。针对每位患者创建并优化了6个PBS计划,使用3种光斑尺寸(等中心处90至230 MeV能量范围的中位标准差分别约为12、5.4和2.5 mm),并在较大光斑尺寸的计划中添加准直器和补偿器。对适形度和均匀性指数、剂量体积直方图参数、等效均匀剂量(EUD)、正常组织并发症概率(NTCP)和积分剂量进行量化,并与各自的PSPT计划进行比较。
结果清楚地表明,使用最大光斑尺寸的PBS不一定比PSPT具有剂量学或临床优势。在靶区覆盖相当的情况下,使用这种光斑尺寸时,健康器官的平均剂量(Dmean)比PSPT平均高6.3%。然而,在大光斑尺寸的计划中添加准直器可提高治疗质量,平均Dmean和EUD分别降低至规定剂量的8.6%和3.2%。进一步减小光斑尺寸可进一步改善所有计划,与PSPT相比,平均Dmean和EUD分别降低至11.6%和10.9%,并无需使用束流整形装置。NTCP随光斑尺寸减小和添加准直器而降低,相对于PSPT最大降低5.4%。
使用PBS的附加益处很大程度上取决于输送配置。对于限于大光斑尺寸(等中心处中位标准差>约8 mm)的设备,建议使用准直器以降低与治疗相关的毒性,至少对于复杂和/或小肿瘤应如此。