Figueroa Jose F, Tsugawa Yusuke, Zheng Jie, Orav E John, Jha Ashish K
Department of Health Policy and Management, Harvard T.H. Chan School of Public Health, Boston, MA 02115, USA Department of Medicine, Brigham and Women's Hospital, Boston, MA, USA.
Department of Health Policy and Management, Harvard T.H. Chan School of Public Health, Boston, MA 02115, USA.
BMJ. 2016 May 9;353:i2214. doi: 10.1136/bmj.i2214.
To determine the impact of the Hospital Value-Based Purchasing (HVBP) program-the US pay for performance program introduced by Medicare to incentivize higher quality care-on 30 day mortality for three incentivized conditions: acute myocardial infarction, heart failure, and pneumonia.
Observational study.
4267 acute care hospitals in the United States: 2919 participated in the HVBP program and 1348 were ineligible and used as controls (44 in general hospitals in Maryland and 1304 critical access hospitals across the United States).
2 430 618 patients admitted to US hospitals from 2008 through 2013.
30 day risk adjusted mortality for acute myocardial infarction, heart failure, and pneumonia using a patient level linear spline analysis to examine the association between the introduction of the HVBP program and 30 day mortality. Non-incentivized, medical conditions were the comparators. A secondary outcome measure was to determine whether the introduction of the HVBP program was particularly beneficial for a subgroup of hospital-poor performers at baseline-that may benefit the most.
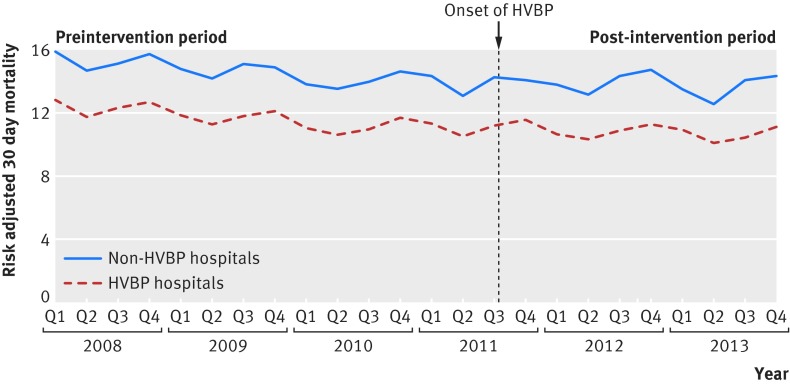
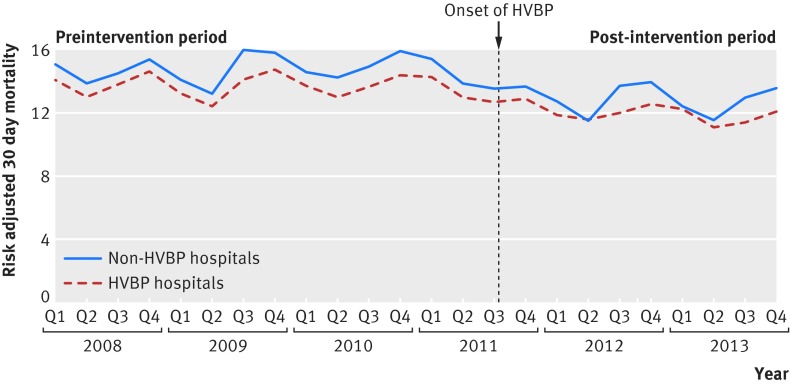
Mortality rates of incentivized conditions in hospitals participating in the HVBP program declined at -0.13% for each quarter during the preintervention period and -0.03% point difference for each quarter during the post-intervention period. For non-HVBP hospitals, mortality rates declined at -0.14% point difference for each quarter during the preintervention period and -0.01% point difference for each quarter during the post-intervention period. The difference in the mortality trends between the two groups was small and non-significant (difference in difference in trends -0.03% point difference for each quarter, 95% confidence interval -0.08% to 0.13% point difference, P=0.35). In no subgroups of hospitals was HVBP associated with better outcomes, including poor performers at baseline.
Evidence that HVBP has led to lower mortality rates is lacking. Nations considering similar pay for performance programs may want to consider alternative models to achieve improved patient outcomes.
确定医院基于价值的购买(HVBP)计划(美国医疗保险推出的按绩效付费计划,旨在激励提供更高质量的医疗服务)对三种激励条件下(急性心肌梗死、心力衰竭和肺炎)30天死亡率的影响。
观察性研究。
美国4267家急性护理医院:2919家参与HVBP计划,1348家不符合条件并用作对照(马里兰州44家综合医院和美国各地1304家急救医院)。
2008年至2013年期间入住美国医院的2430618名患者。
使用患者水平线性样条分析来检查HVBP计划的引入与30天死亡率之间的关联,以得出急性心肌梗死、心力衰竭和肺炎的30天风险调整死亡率。非激励性医疗状况作为对照。次要观察指标是确定HVBP计划的引入是否对基线时表现较差的医院亚组特别有益,因为这些医院可能受益最大。
参与HVBP计划的医院中,激励条件下的死亡率在干预前期每季度下降-0.13%,在干预后期每季度下降-0.03个百分点。对于非HVBP医院,死亡率在干预前期每季度下降-0.14个百分点,在干预后期每季度下降-0.01个百分点。两组死亡率趋势的差异很小且无统计学意义(趋势差异的差异为每季度-0.03个百分点,95%置信区间为-0.08%至0.13个百分点,P=0.35)。在任何医院亚组中,HVBP均未与更好的结果相关,包括基线时表现较差的医院。
缺乏证据表明HVBP导致了更低的死亡率。考虑类似按绩效付费计划的国家可能需要考虑替代模式以改善患者结局。