Wallentin Lars, Held Claes, Armstrong Paul W, Cannon Christopher P, Davies Richard Y, Granger Christopher B, Hagström Emil, Harrington Robert A, Hochman Judith S, Koenig Wolfgang, Krug-Gourley Sue, Mohler Emile R, Siegbahn Agneta, Tarka Elizabeth, Steg Philippe Gabriel, Stewart Ralph A H, Weiss Robert, Östlund Ollie, White Harvey D
Department of Medical Sciences, Cardiology, Uppsala University, Uppsala, Sweden Uppsala Clinical Research Center (UCR), Uppsala University, Uppsala, Sweden
Department of Medical Sciences, Cardiology, Uppsala University, Uppsala, Sweden Uppsala Clinical Research Center (UCR), Uppsala University, Uppsala, Sweden.
J Am Heart Assoc. 2016 Jun 21;5(6):e003407. doi: 10.1161/JAHA.116.003407.
We evaluated lipoprotein-associated phospholipase A2 (Lp-PLA2) activity in patients with stable coronary heart disease before and during treatment with darapladib, a selective Lp-PLA2 inhibitor, in relation to outcomes and the effects of darapladib in the STABILITY trial.
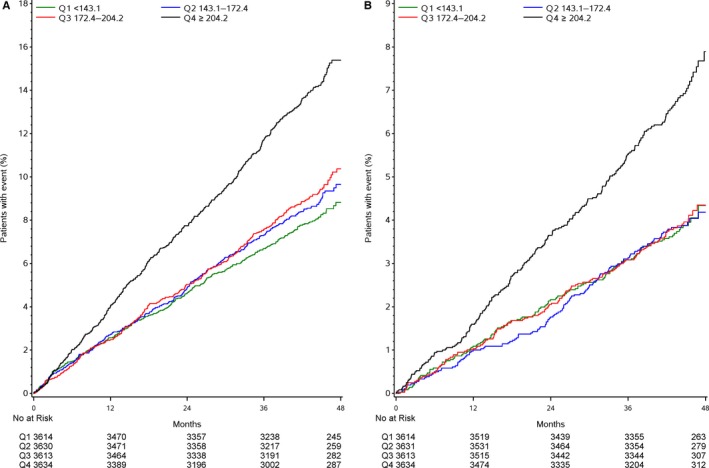
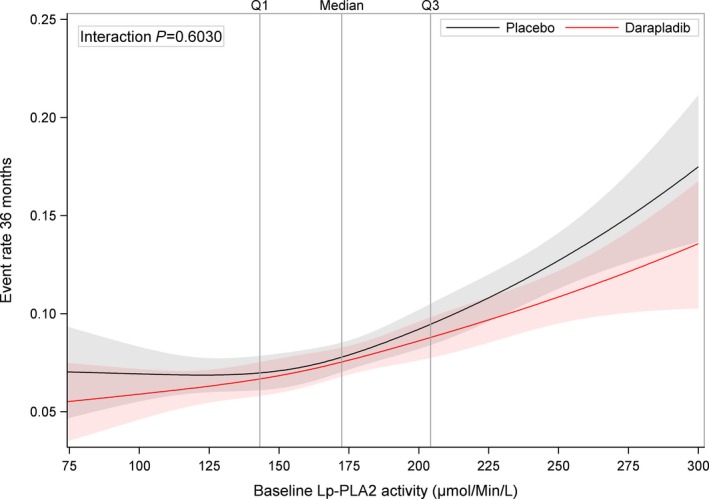
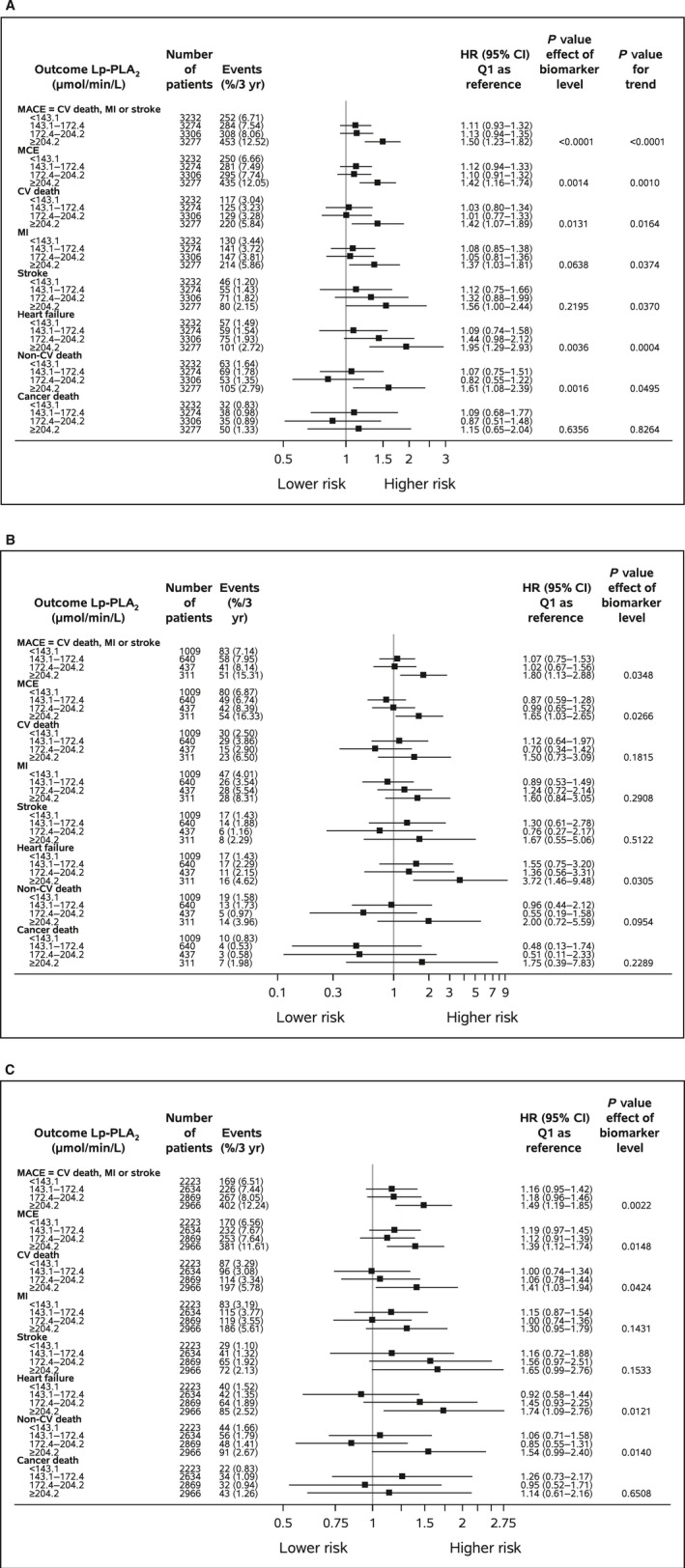
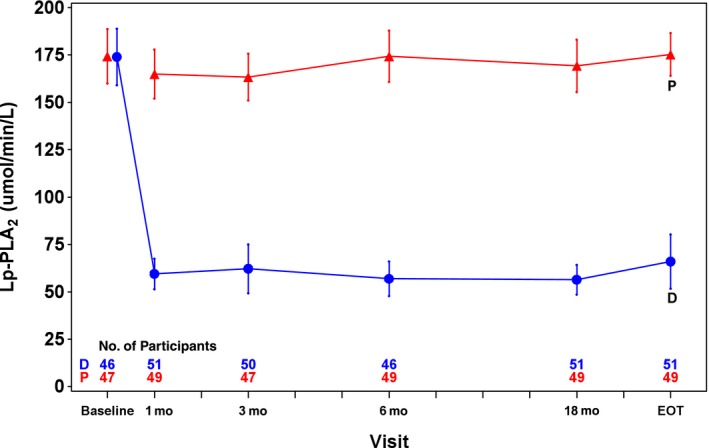
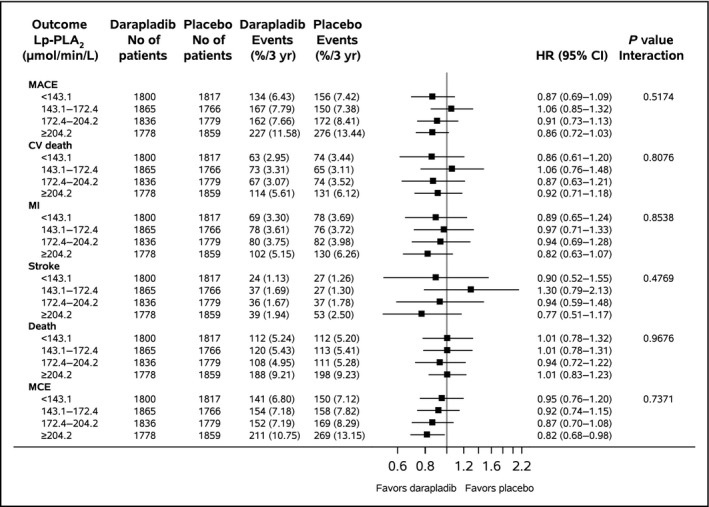
Plasma Lp-PLA2 activity was determined at baseline (n=14 500); at 1 month (n=13 709); serially (n=100) at 3, 6, and 18 months; and at the end of treatment. Adjusted Cox regression models evaluated associations between Lp-PLA2 activity levels and outcomes. At baseline, the median Lp-PLA2 level was 172.4 μmol/min per liter (interquartile range 143.1-204.2 μmol/min per liter). Comparing the highest and lowest Lp-PLA2 quartile groups, the hazard ratios were 1.50 (95% CI 1.23-1.82) for the primary composite end point (cardiovascular death, myocardial infarction, or stroke), 1.95 (95% CI 1.29-2.93) for hospitalization for heart failure, 1.42 (1.07-1.89) for cardiovascular death, and 1.37 (1.03-1.81) for myocardial infarction after adjustment for baseline characteristics, standard laboratory variables, and other prognostic biomarkers. Treatment with darapladib led to a ≈65% persistent reduction in median Lp-PLA2 activity. There were no associations between on-treatment Lp-PLA2 activity or changes of Lp-PLA2 activity and outcomes, and there were no significant interactions between baseline and on-treatment Lp-PLA2 activity or changes in Lp-PLA2 activity levels and the effects of darapladib on outcomes.
Although high Lp-PLA2 activity was associated with increased risk of cardiovascular events, pharmacological lowering of Lp-PLA2 activity by ≈65% did not significantly reduce cardiovascular events in patients with stable coronary heart disease, regardless of the baseline level or the magnitude of change of Lp-PLA2 activity.
URL: https://www.clinicaltrials.gov. Unique identifier: NCT00799903.
在稳定性试验(STABILITY trial)中,我们评估了脂蛋白相关磷脂酶A2(Lp-PLA2)抑制剂达帕利单抗治疗前及治疗期间,稳定型冠心病患者的Lp-PLA2活性与预后以及达帕利单抗疗效之间的关系。
在基线时(n = 14500)、1个月时(n = 13709)、3个月、6个月和18个月时连续(n = 100)以及治疗结束时测定血浆Lp-PLA2活性。采用校正后的Cox回归模型评估Lp-PLA2活性水平与预后之间的关联。在基线时,Lp-PLA2的中位数水平为172.4 μmol/min per liter(四分位间距为143.1 - 204.2 μmol/min per liter)。比较Lp-PLA2最高和最低四分位组,在校正基线特征、标准实验室变量和其他预后生物标志物后,主要复合终点(心血管死亡、心肌梗死或中风)的风险比为1.50(95%CI 1.23 - 1.82),因心力衰竭住院的风险比为1.95(95%CI 1.29 - 2.93),心血管死亡的风险比为1.42(1.07 - 1.89),心肌梗死的风险比为1.37(1.03 - 1.81)。达帕利单抗治疗使Lp-PLA2活性中位数持续降低约65%。治疗期间的Lp-PLA2活性或Lp-PLA2活性变化与预后之间无关联,基线和治疗期间的Lp-PLA2活性或Lp-PLA2活性水平变化与达帕利单抗对预后的影响之间无显著交互作用。
尽管高Lp-PLA2活性与心血管事件风险增加相关,但无论Lp-PLA2活性的基线水平或变化幅度如何,通过药物使Lp-PLA2活性降低约65%并不能显著降低稳定型冠心病患者的心血管事件。