Le Bourgeois Muriel, Ferroni Agnès, Leruez-Ville Marianne, Varon Emmanuelle, Thumerelle Caroline, Brémont François, Fayon Michael J, Delacourt Christophe, Ligier Caroline, Watier Laurence, Guillemot Didier
Department of Pediatric Pulmonology, University Hospital Necker-Enfants Malades, APHP, Paris, France.
Department of Microbiology, University Hospital Necker-Enfants Malades, APHP, Paris, France.
J Pediatr. 2016 Aug;175:47-53.e3. doi: 10.1016/j.jpeds.2016.05.025. Epub 2016 Jun 20.
To investigate the risk factors of empyema after acute viral infection and to clarify the hypothesized association(s) between empyema and some viruses and/or the use of nonsteroidal anti-inflammatory drugs (NSAIDs).
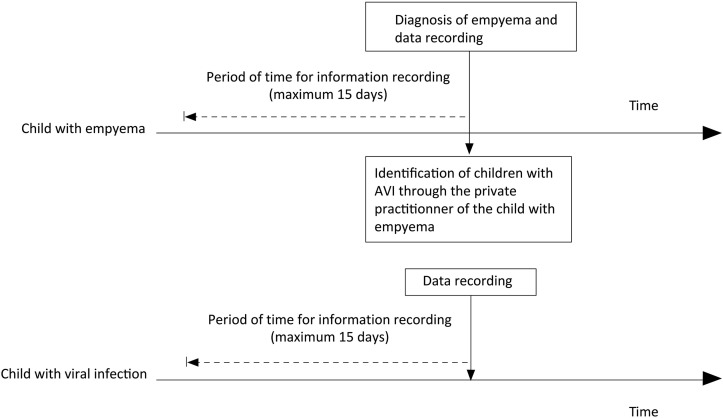
A case-control study was conducted in 15 centers. Cases and controls were enrolled for a source population of children 3-15 years of age with acute viral infections between 2006 and 2009.
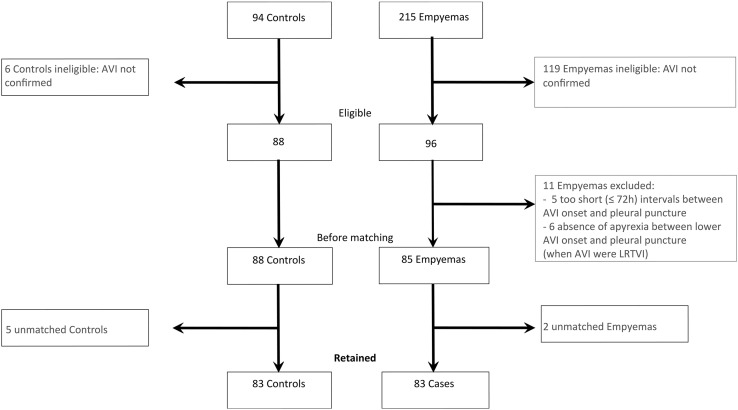
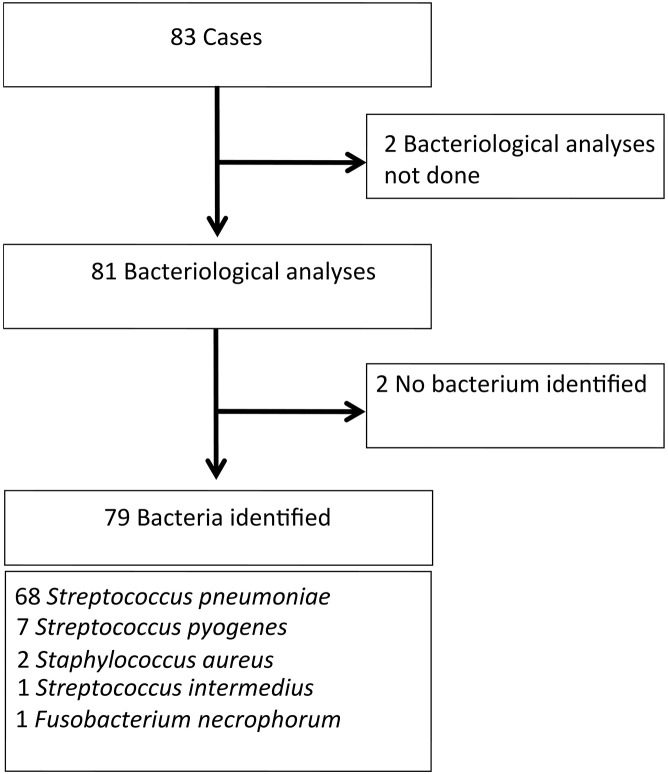
Among 215 empyemas, 83 cases (children with empyema and acute viral infection within the 15 preceding days) were included, and 83 controls (children with acute viral infection) were matched to cases. Considering the intake of any drug within 72 hours after acute viral infection onset and at least 6 consecutive days of antibiotic use and at least 1 day of NSAIDs exposure, the multivariable analysis retained an increased risk of empyema associated with NSAIDs exposure (aOR 2.79, 95% CI 1.4-5.58, P = .004), and a decreased risk associated with antibiotic use (aOR 0.32, 95% CI 0.11-0.97, P = .04). The risk of empyema associated with NSAIDs exposure was greater for children not prescribed an antibiotic and antibiotic intake diminished that risk for children given NSAIDs.
NSAIDs use during acute viral infection is associated with an increased risk of empyema in children, and antibiotics are associated with a decreased risk. The presence of antibiotic-NSAIDs interaction with this risk is suggested. These findings suggest that NSAIDs should not be recommended as a first-line antipyretic treatment during acute viral infections in children.
探讨急性病毒感染后发生脓胸的危险因素,并阐明脓胸与某些病毒和/或使用非甾体抗炎药(NSAIDs)之间的假定关联。
在15个中心进行了一项病例对照研究。病例和对照来自2006年至2009年期间3至15岁患有急性病毒感染的儿童源人群。
在215例脓胸病例中,纳入了83例(在过去15天内患有脓胸和急性病毒感染的儿童),并将83例对照(患有急性病毒感染的儿童)与病例进行匹配。考虑到急性病毒感染发病后72小时内使用的任何药物、至少连续6天使用抗生素以及至少1天接触NSAIDs,多变量分析显示,接触NSAIDs会增加脓胸风险(调整后比值比[aOR]为2.79,95%置信区间[CI]为1.4 - 5.58,P = 0.004),而使用抗生素会降低脓胸风险(aOR为0.32,95% CI为0.11 - 0.97,P = 0.04)。未开具抗生素处方的儿童接触NSAIDs导致脓胸的风险更高,而抗生素摄入可降低使用NSAIDs儿童的该风险。
儿童急性病毒感染期间使用NSAIDs会增加脓胸风险,而使用抗生素则会降低脓胸风险。提示存在抗生素 - NSAIDs与该风险的相互作用。这些发现表明,在儿童急性病毒感染期间,不应推荐将NSAIDs作为一线退热治疗药物。