Kristensen Søren Lund, Martinez Felipe, Jhund Pardeep S, Arango Juan Luis, Bĕlohlávek Jan, Boytsov Sergey, Cabrera Walter, Gomez Efrain, Hagège Albert A, Huang Jun, Kiatchoosakun Songsak, Kim Kee-Sik, Mendoza Iván, Senni Michele, Squire Iain B, Vinereanu Dragos, Wong Raymond Ching-Chiew, Gong Jianjian, Lefkowitz Martin P, Rizkala Adel R, Rouleau Jean L, Shi Victor C, Solomon Scott D, Swedberg Karl, Zile Michael R, Packer Milton, McMurray John J V
BHF Glasgow Cardiovascular Research Centre, Institute of Cardiovascular and Medical Sciences, University of Glasgow, Glasgow G12 8TA, UK
Department of Cardiology, Rigshospitalet, Copenhagen, Denmark.
Eur Heart J. 2016 Nov 1;37(41):3167-3174. doi: 10.1093/eurheartj/ehw226. Epub 2016 Jun 28.
The globalization of clinical trials has highlighted geographic variations in patient characteristics, event rates, and treatment effects. We investigated these further in PARADIGM-HF, the largest and most globally representative trial in heart failure (HF) to date.
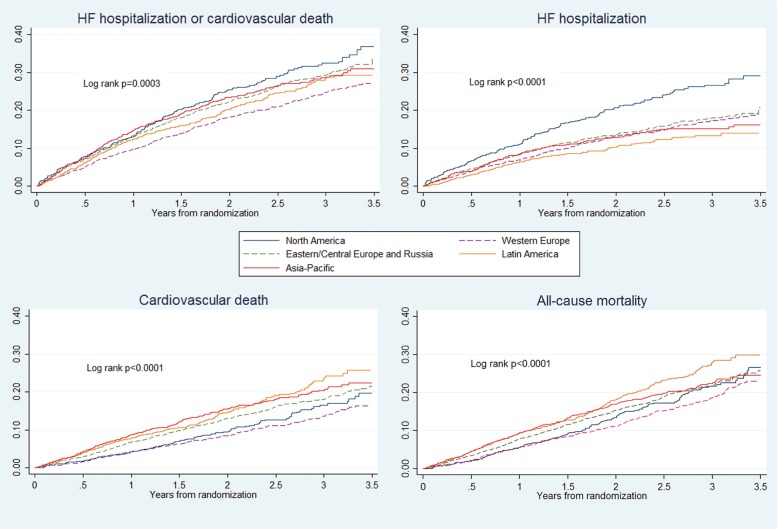
We looked at five regions: North America (NA) 602 (8%), Western Europe (WE) 1680 (20%), Central/Eastern Europe/Russia (CEER) 2762 (33%), Latin America (LA) 1433 (17%), and Asia-Pacific (AP) 1487 (18%). Notable differences included: WE patients (mean age 68 years) and NA (65 years) were older than AP (58 years) and LA (63 years) and had more coronary disease; NA and CEER patients had the worst signs, symptoms, and functional status. North American patients were the most likely to have a defibrillating-device (54 vs. 2% AP) and least likely prescribed a mineralocorticoid receptor antagonist (36 vs. 65% LA). Other evidence-based therapies were used most frequently in NA and WE. Rates of the primary composite outcome of cardiovascular (CV) death or HF hospitalization (per 100 patient-years) varied among regions: NA 13.6 (95% CI 11.7-15.7) WE 9.6 (8.6-10.6), CEER 12.3 (11.4-13.2), LA 11.2 (10.0-12.5), and AP 12.5 (11.3-13.8). After adjustment for prognostic variables, relative to NA, the risk of CV death was higher in LA and AP and the risk of HF hospitalization lower in WE. The benefit of sacubitril/valsartan was consistent across regions.
There were many regional differences in PARADIGM-HF, including in age, symptoms, comorbidity, background therapy, and event-rates, although these did not modify the benefit of sacubitril/valsartan. CLINICAL TRIAL REGISTRATION URL: http://www.clinicaltrials.gov. Unique identifier: NCT01035255.
临床试验的全球化凸显了患者特征、事件发生率和治疗效果的地域差异。我们在PARADIGM-HF研究中对此进行了进一步调查,这是迄今为止规模最大且最具全球代表性的心力衰竭(HF)试验。
我们观察了五个地区:北美(NA)602例(8%)、西欧(WE)1680例(20%)、中东欧/俄罗斯(CEER)2762例(33%)、拉丁美洲(LA)1433例(17%)以及亚太地区(AP)1487例(18%)。显著差异包括:西欧患者(平均年龄68岁)和北美患者(65岁)比亚太地区患者(58岁)和拉丁美洲患者(63岁)年龄更大,且冠心病更多;北美和中东欧/俄罗斯患者的体征、症状和功能状态最差。北美患者最有可能植入除颤装置(54%对比亚太地区的2%),且最不可能开具盐皮质激素受体拮抗剂(36%对比拉丁美洲的65%)。其他循证疗法在北美和西欧使用最为频繁。心血管(CV)死亡或HF住院的主要复合结局发生率(每100患者年)在各地区有所不同:北美为13.6(95%CI 11.7 - 15.7),西欧为9.6(8.6 - 10.6),中东欧/俄罗斯为12.3(11.4 - 13.2),拉丁美洲为11.2(10.0 - 12.5),亚太地区为12.5(11.3 - 13.8)。在对预后变量进行调整后,相对于北美,拉丁美洲和亚太地区CV死亡风险更高,而西欧HF住院风险更低。沙库巴曲缬沙坦的获益在各地区是一致的。
PARADIGM-HF研究存在许多地区差异,包括年龄、症状、合并症、背景治疗和事件发生率等方面,尽管这些并未改变沙库巴曲缬沙坦的获益。临床试验注册网址:http://www.clinicaltrials.gov。唯一标识符:NCT01035255。