Ortiz Mercedes, Martín Alfonso, Arribas Fernando, Coll-Vinent Blanca, Del Arco Carmen, Peinado Rafael, Almendral Jesús
Department of Cardiology, Hospital General Universitario Gregorio Marañón, Madrid, Spain.
Emergency Department, Hospital Universitario Severo Ochoa, Madrid, Spain.
Eur Heart J. 2017 May 1;38(17):1329-1335. doi: 10.1093/eurheartj/ehw230.
Intravenous procainamide and amiodarone are drugs of choice for well-tolerated ventricular tachycardia. However, the choice between them, even according to Guidelines, is unclear. We performed a multicentre randomized open-labelled study to determine the safety and efficacy of intravenous procainamide and amiodarone for the acute treatment of tolerated wide QRS complex (probably ventricular) tachycardia.
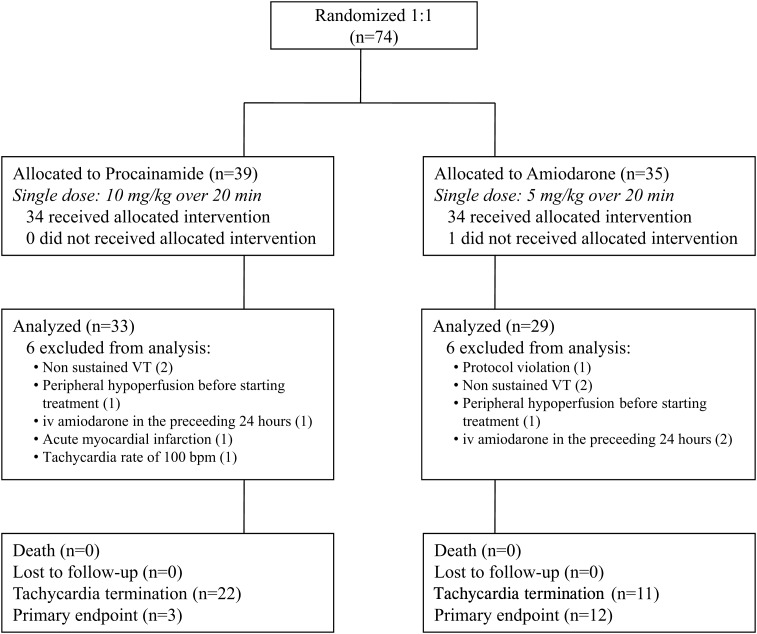
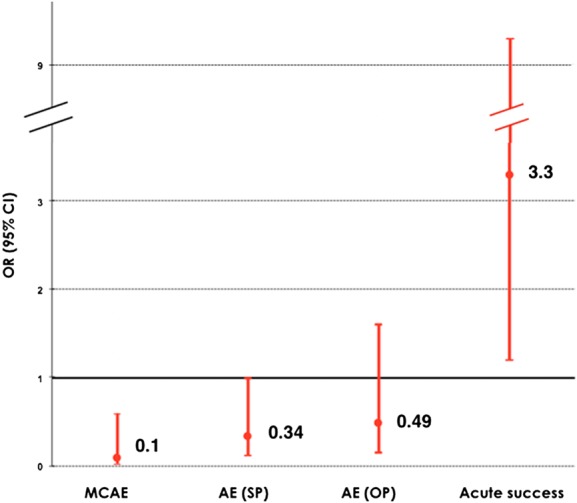
Patients were randomly assigned to receive intravenous procainamide (10 mg/kg/20 min) or amiodarone (5 mg/kg/20 min). The primary endpoint was the incidence of major predefined cardiac adverse events within 40 min after infusion initiation. Of 74 patients included, 62 could be analysed. The primary endpoint occurred in 3 of 33 (9%) procainamide and 12 of 29 (41%) amiodarone patients (odd ratio, OR = 0.1; 95% confidence interval, CI 0.03-0.6; P = 0.006). Tachycardia terminated within 40 min in 22 (67%) procainamide and 11 (38%) amiodarone patients (OR = 3.3; 95% CI 1.2-9.3; P = 0.026). In the following 24 h, adverse events occurred in 18% procainamide and 31% amiodarone patients (OR: 0.49; 95% CI: 0.15-1.61; P: 0.24). Among 49 patients with structural heart disease, the primary endpoint was less common in procainamide patients (3 [11%] vs. 10 [43%]; OR: 0.17; 95% CI: 0.04-0.73, P = 0.017).
This study compares for the first time in a randomized design intravenous procainamide and amiodarone for the treatment of the acute episode of sustained monomorphic well-tolerated (probably) ventricular tachycardia. Procainamide therapy was associated with less major cardiac adverse events and a higher proportion of tachycardia termination within 40 min.
静脉注射普鲁卡因胺和胺碘酮是耐受性良好的室性心动过速的首选药物。然而,即使根据指南,在它们之间进行选择也不明确。我们开展了一项多中心随机开放标签研究,以确定静脉注射普鲁卡因胺和胺碘酮用于急性治疗耐受性良好的宽QRS波群(可能为室性)心动过速的安全性和有效性。
患者被随机分配接受静脉注射普鲁卡因胺(10mg/kg/20分钟)或胺碘酮(5mg/kg/20分钟)。主要终点是输注开始后40分钟内主要预先定义的心脏不良事件的发生率。纳入的74例患者中,62例可进行分析。主要终点在33例接受普鲁卡因胺治疗的患者中有3例(9%)出现,在29例接受胺碘酮治疗的患者中有12例(41%)出现(比值比,OR = 0.1;95%置信区间,CI 0.03 - 0.6;P = 0.006)。22例(67%)接受普鲁卡因胺治疗的患者和11例(38%)接受胺碘酮治疗的患者心动过速在40分钟内终止(OR = 3.3;95% CI 1.2 - 9.3;P = 0.026)。在接下来的24小时内,18%接受普鲁卡因胺治疗的患者和31%接受胺碘酮治疗的患者出现不良事件(OR:0.49;95% CI:0.15 - 1.61;P:0.24)。在49例患有结构性心脏病的患者中,主要终点在接受普鲁卡因胺治疗的患者中较少见(3例[11%]对10例[43%];OR:0.17;95% CI:0.04 - 0.73,P = 0.017)。
本研究首次在随机设计中比较了静脉注射普鲁卡因胺和胺碘酮治疗持续性单形性耐受性良好(可能为)室性心动过速的急性发作。普鲁卡因胺治疗与较少的主要心脏不良事件以及40分钟内更高比例的心动过速终止相关。