van Beuge Marike M, Ten Dam Evert-Jan P M, Werker Paul M N, Bank Ruud A
Department of Pathology & Medical Biology, University Medical Center Groningen, University of Groningen, Hanzeplein 1, 9713 GZ Groningen, The Netherlands.
Department of Pathology & Medical Biology, University Medical Center Groningen, University of Groningen, Hanzeplein 1, 9713 GZ Groningen, The Netherlands ; Department of Plastic Surgery, Department of Pathology & Medical Biology, University Medical Center Groningen, University of Groningen, Hanzeplein 1, 9713 GZ Groningen, The Netherlands.
Fibrogenesis Tissue Repair. 2016 Jun 29;9:9. doi: 10.1186/s13069-016-0046-0. eCollection 2016.
Dupuytren's disease is a fibroproliferative disease of the hand and fingers, which usually manifests as two different phenotypes within the same patient. The disease first causes a nodule in the palm of the hand, while later, a cord develops, causing contracture of the fingers.
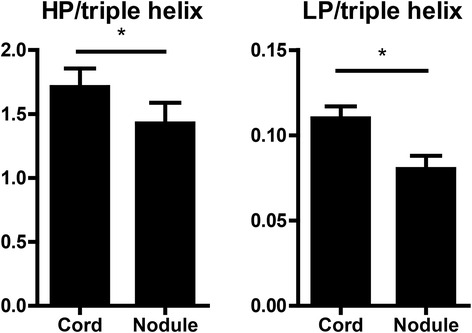
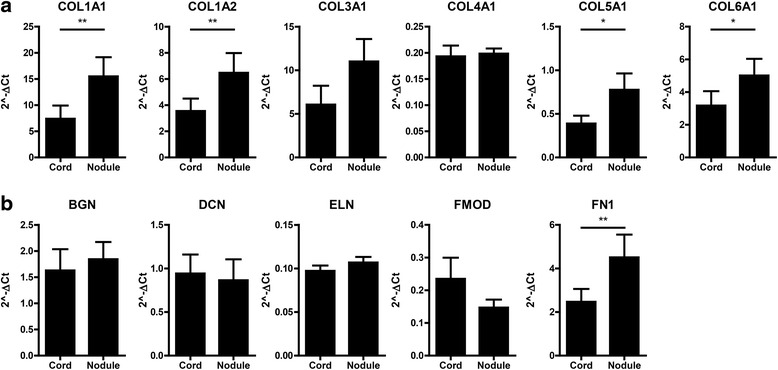
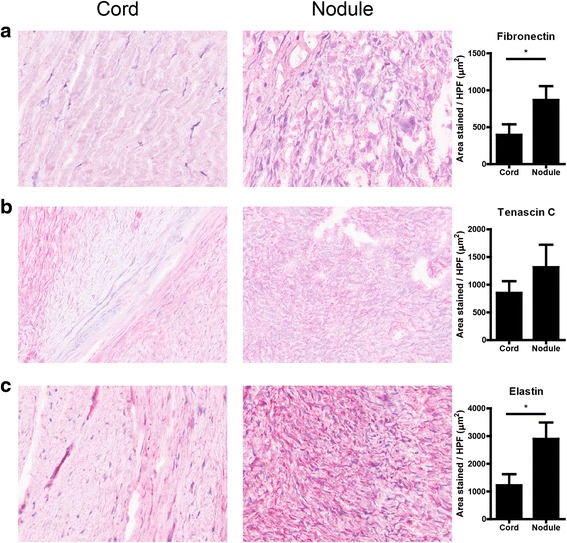
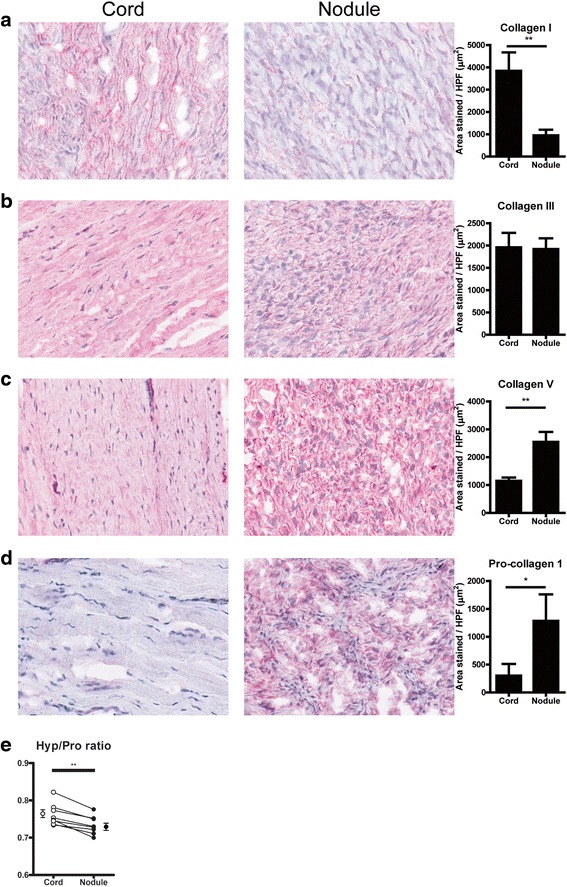
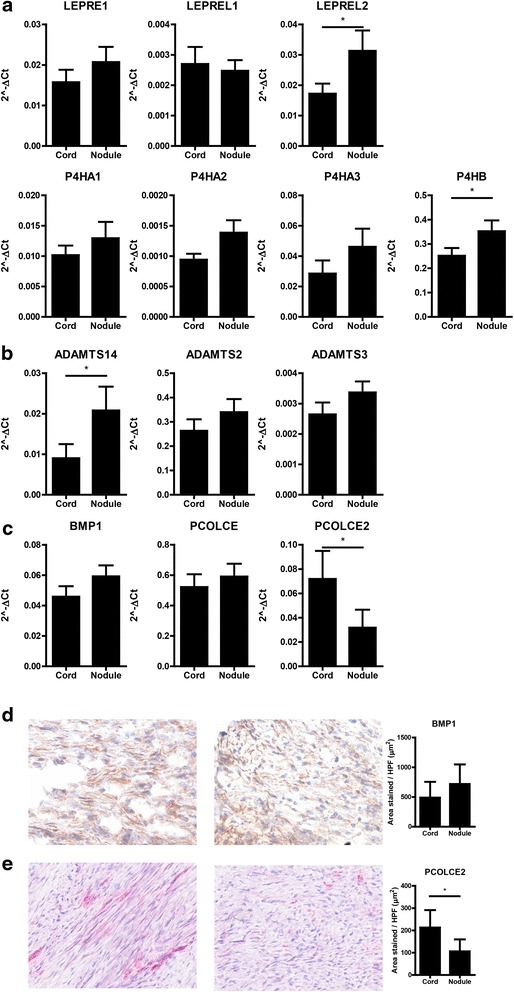
We set out to characterize the two phenotypes by comparing matched cord and nodule tissue from ten Dupuytren's patients. We found that nodule tissue contained more proliferating cells, CD68-positive macrophages and α-smooth muscle actin (α-SMA)-positive myofibroblastic cells. qPCR analysis showed an increased expression of COL1A1, COL1A2, COL5A1, and COL6A1 in nodule tissue compared to cord tissue. Immunohistochemistry showed less deposition of collagen type I in nodules, although they contained more fibronectin, collagen type V, and procollagen 1. Lower collagen levels in nodule were confirmed by HPLC measurements of the Hyp/Pro ratio. PCOLCE2, an activator of BMP1, the main enzyme cleaving the C-terminal pro-peptide from procollagen, was also reduced in nodule. Cord tissue not only contained more collagen I, but also higher levels of hydroxylysylpyridinoline and lysylpyridinoline residues per triple helix, indicating more crosslinks.
Our results clearly show that in Dupuytren's disease, the nodule is the active disease unit, although it does not have the highest collagen protein levels. The difference in collagen type I deposition compared to mRNA levels and procollagen 1 levels may be connected to a decrease in procollagen processing.
杜普伊特伦挛缩病是一种手部和手指的纤维增生性疾病,通常在同一患者体内表现为两种不同的表型。该病首先在手掌形成一个结节,随后形成条索,导致手指挛缩。
我们通过比较10例杜普伊特伦挛缩病患者匹配的条索和结节组织来表征这两种表型。我们发现结节组织含有更多的增殖细胞、CD68阳性巨噬细胞和α平滑肌肌动蛋白(α-SMA)阳性肌成纤维细胞。qPCR分析显示,与条索组织相比,结节组织中COL1A1、COL1A2、COL5A1和COL6A1的表达增加。免疫组织化学显示结节中I型胶原蛋白的沉积较少,尽管它们含有更多的纤连蛋白、V型胶原蛋白和前胶原蛋白1。通过HPLC测量Hyp/Pro比值证实结节中的胶原蛋白水平较低。PCOLCE2是BMP1的激活剂,BMP1是从前胶原蛋白切割C末端前肽的主要酶,在结节中也减少。条索组织不仅含有更多的I型胶原蛋白,而且每条三螺旋中羟赖氨酸吡啶啉和赖氨酸吡啶啉残基的水平也更高,表明交联更多。
我们的结果清楚地表明,在杜普伊特伦挛缩病中,结节是活跃的疾病单位,尽管它的胶原蛋白蛋白水平不是最高的。I型胶原蛋白沉积与mRNA水平和前胶原蛋白1水平的差异可能与前胶原蛋白加工减少有关。